Benson Nasasira, Grace Banturaki, Nelson Kalema, Joseph Musaazi, Aidah Nanvuma, Stephen Okoboi, Nancy Gathoni Kiarie, Joash Ntenga Moitui, Damazo Kadengye, Jonathan Izudi, Barbara Castelnuovo
{"title":"差异化服务提供模式对乌干达艾滋病毒感染者生活质量的影响——一项准实验研究。","authors":"Benson Nasasira, Grace Banturaki, Nelson Kalema, Joseph Musaazi, Aidah Nanvuma, Stephen Okoboi, Nancy Gathoni Kiarie, Joash Ntenga Moitui, Damazo Kadengye, Jonathan Izudi, Barbara Castelnuovo","doi":"10.1186/s12981-025-00741-9","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Differentiated service delivery (DSD) models in resource-limited settings reduce strain on health services and improve clinical outcomes such as retention and viral suppression, but little is known about the impact of HIV DSD models on quality of life (QoL), which is essential for optimizing person-centered care. This study assessed the impact of DSD models on Quality of life, loss to follow-up (LTFU), and mortality among persons living with HIV (PLHIV) on Antiretroviral therapy (ART) over time at a large urban HIV clinic in Uganda.</p><p><strong>Methods: </strong>Records of 1,000 PLHIV enrolled in a 10-year cohort at the Infectious Diseases Institute (IDI) clinic in Kampala, Uganda were retrospectively analyzed. QoL was assessed using an adapted Medical Outcomes Study (MOS-HIV) tool. QoL scores, sustained annual viral suppression (< 200 copies/mL), all-cause mortality and LTFU (≥ 3 months of missed visits) were compared for PLHIV in three DSD models for ≥ 6 consecutive months-fast-track drug refill (FTDR), facility-based groups (FBG), and composite model combining these two-versus facility-based individual management (FBIM) or the standard of care (SOC). Inverse probability treatment weighting was applied for covariate comparability while robustness of results was checked using G-computation. Sustained viral suppression was compared using odds ratios; all-cause mortality and LTFU were compared using hazard ratios from the Cox proportional hazard regression model.</p><p><strong>Results: </strong>Of the 1,000 PLHIV, 980 had ≥ 1 follow-up and were included in the analysis. Median age was 45 years (IQR: 40-51), 62% were female, and 95% had a suppressed viral load at baseline. Baseline QoL was 90.1% in any DSD model vs. 89.2% in SOC. After eight years of follow-up, weighted mean QoL was higher in participants enrolled in DSD models than the SOC (90.4% vs. 89.1%; weighted mean ratio 3.66, 95% CI 2.10-6.37, p-value < 0.001); there were no statistical differences across DSD models. Participants in DSD models were more likely to have sustained viral suppression (weighted odds ratio 1.69, 95% CI 1.24-2.31), lower mortality (weighted hazard ratio 0.08, 95% CI 0.03-0.20) and lower LTFU rates (weighted hazard ratio 0.08, 95% CI 0.02-0.31).</p><p><strong>Conclusion: </strong>DSD models were associated with modestly higher quality of life, better viral suppression, and lower mortality and LTFU compared to the standard of care. These findings support the broader adoption of DSD models in delivering ART across HIV programs to enhance the QoL and clinical outcomes among PLHIV.</p>","PeriodicalId":7503,"journal":{"name":"AIDS Research and Therapy","volume":"22 1","pages":"56"},"PeriodicalIF":2.5000,"publicationDate":"2025-06-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12128276/pdf/","citationCount":"0","resultStr":"{\"title\":\"Impact of differentiated service delivery models on quality of life among people living with HIV in Uganda- a quasi-experimental study.\",\"authors\":\"Benson Nasasira, Grace Banturaki, Nelson Kalema, Joseph Musaazi, Aidah Nanvuma, Stephen Okoboi, Nancy Gathoni Kiarie, Joash Ntenga Moitui, Damazo Kadengye, Jonathan Izudi, Barbara Castelnuovo\",\"doi\":\"10.1186/s12981-025-00741-9\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Differentiated service delivery (DSD) models in resource-limited settings reduce strain on health services and improve clinical outcomes such as retention and viral suppression, but little is known about the impact of HIV DSD models on quality of life (QoL), which is essential for optimizing person-centered care. This study assessed the impact of DSD models on Quality of life, loss to follow-up (LTFU), and mortality among persons living with HIV (PLHIV) on Antiretroviral therapy (ART) over time at a large urban HIV clinic in Uganda.</p><p><strong>Methods: </strong>Records of 1,000 PLHIV enrolled in a 10-year cohort at the Infectious Diseases Institute (IDI) clinic in Kampala, Uganda were retrospectively analyzed. QoL was assessed using an adapted Medical Outcomes Study (MOS-HIV) tool. QoL scores, sustained annual viral suppression (< 200 copies/mL), all-cause mortality and LTFU (≥ 3 months of missed visits) were compared for PLHIV in three DSD models for ≥ 6 consecutive months-fast-track drug refill (FTDR), facility-based groups (FBG), and composite model combining these two-versus facility-based individual management (FBIM) or the standard of care (SOC). Inverse probability treatment weighting was applied for covariate comparability while robustness of results was checked using G-computation. Sustained viral suppression was compared using odds ratios; all-cause mortality and LTFU were compared using hazard ratios from the Cox proportional hazard regression model.</p><p><strong>Results: </strong>Of the 1,000 PLHIV, 980 had ≥ 1 follow-up and were included in the analysis. Median age was 45 years (IQR: 40-51), 62% were female, and 95% had a suppressed viral load at baseline. Baseline QoL was 90.1% in any DSD model vs. 89.2% in SOC. After eight years of follow-up, weighted mean QoL was higher in participants enrolled in DSD models than the SOC (90.4% vs. 89.1%; weighted mean ratio 3.66, 95% CI 2.10-6.37, p-value < 0.001); there were no statistical differences across DSD models. Participants in DSD models were more likely to have sustained viral suppression (weighted odds ratio 1.69, 95% CI 1.24-2.31), lower mortality (weighted hazard ratio 0.08, 95% CI 0.03-0.20) and lower LTFU rates (weighted hazard ratio 0.08, 95% CI 0.02-0.31).</p><p><strong>Conclusion: </strong>DSD models were associated with modestly higher quality of life, better viral suppression, and lower mortality and LTFU compared to the standard of care. These findings support the broader adoption of DSD models in delivering ART across HIV programs to enhance the QoL and clinical outcomes among PLHIV.</p>\",\"PeriodicalId\":7503,\"journal\":{\"name\":\"AIDS Research and Therapy\",\"volume\":\"22 1\",\"pages\":\"56\"},\"PeriodicalIF\":2.5000,\"publicationDate\":\"2025-06-02\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12128276/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"AIDS Research and Therapy\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1186/s12981-025-00741-9\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"INFECTIOUS DISEASES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"AIDS Research and Therapy","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s12981-025-00741-9","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"INFECTIOUS DISEASES","Score":null,"Total":0}
引用次数: 0
摘要
背景:在资源有限的环境下,差异化服务提供(DSD)模式减少了卫生服务的压力,改善了临床结果,如保留和病毒抑制,但对艾滋病毒DSD模式对生活质量(QoL)的影响知之甚少,这对于优化以人为本的护理至关重要。本研究评估了DSD模型对生活质量的影响,随访损失(LTFU)和艾滋病毒感染者(PLHIV)抗逆转录病毒治疗(ART)的死亡率随时间的变化。方法:回顾性分析乌干达坎帕拉传染病研究所(IDI)诊所10年队列中1000例PLHIV患者的记录。生活质量的评估使用了一种改编的医疗结果研究(MOS-HIV)工具。生活质量评分,持续的年度病毒抑制(结果:在1000名PLHIV患者中,980例随访≥1次,并被纳入分析。中位年龄为45岁(IQR: 40-51), 62%为女性,95%在基线时病毒载量被抑制。任何DSD模型的基线生活质量为90.1%,而SOC模型为89.2%。经过8年的随访,DSD模型参与者的加权平均生活质量高于SOC (90.4% vs 89.1%;加权平均比值3.66,95% CI 2.10-6.37, p值结论:与标准护理相比,DSD模型与较高的生活质量、较好的病毒抑制、较低的死亡率和LTFU相关。这些发现支持在艾滋病毒项目中更广泛地采用DSD模型提供抗逆转录病毒治疗,以提高艾滋病毒感染者的生活质量和临床结果。
Impact of differentiated service delivery models on quality of life among people living with HIV in Uganda- a quasi-experimental study.
Background: Differentiated service delivery (DSD) models in resource-limited settings reduce strain on health services and improve clinical outcomes such as retention and viral suppression, but little is known about the impact of HIV DSD models on quality of life (QoL), which is essential for optimizing person-centered care. This study assessed the impact of DSD models on Quality of life, loss to follow-up (LTFU), and mortality among persons living with HIV (PLHIV) on Antiretroviral therapy (ART) over time at a large urban HIV clinic in Uganda.
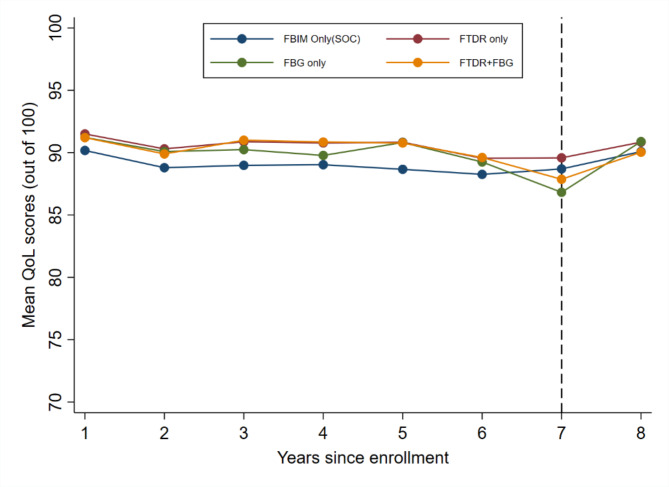
Methods: Records of 1,000 PLHIV enrolled in a 10-year cohort at the Infectious Diseases Institute (IDI) clinic in Kampala, Uganda were retrospectively analyzed. QoL was assessed using an adapted Medical Outcomes Study (MOS-HIV) tool. QoL scores, sustained annual viral suppression (< 200 copies/mL), all-cause mortality and LTFU (≥ 3 months of missed visits) were compared for PLHIV in three DSD models for ≥ 6 consecutive months-fast-track drug refill (FTDR), facility-based groups (FBG), and composite model combining these two-versus facility-based individual management (FBIM) or the standard of care (SOC). Inverse probability treatment weighting was applied for covariate comparability while robustness of results was checked using G-computation. Sustained viral suppression was compared using odds ratios; all-cause mortality and LTFU were compared using hazard ratios from the Cox proportional hazard regression model.
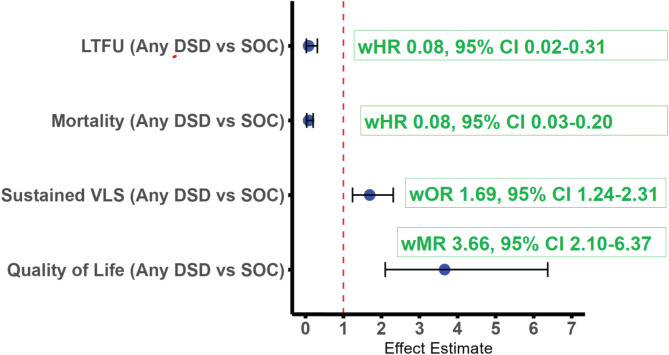
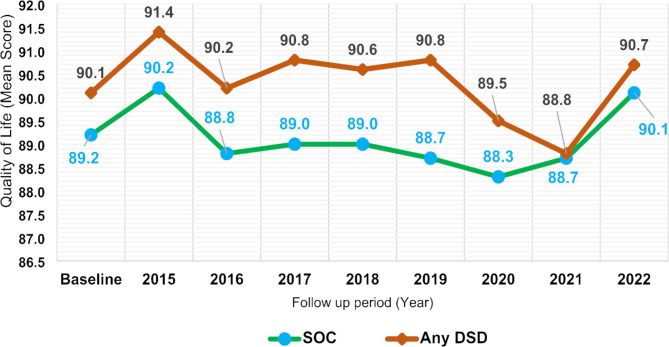
Results: Of the 1,000 PLHIV, 980 had ≥ 1 follow-up and were included in the analysis. Median age was 45 years (IQR: 40-51), 62% were female, and 95% had a suppressed viral load at baseline. Baseline QoL was 90.1% in any DSD model vs. 89.2% in SOC. After eight years of follow-up, weighted mean QoL was higher in participants enrolled in DSD models than the SOC (90.4% vs. 89.1%; weighted mean ratio 3.66, 95% CI 2.10-6.37, p-value < 0.001); there were no statistical differences across DSD models. Participants in DSD models were more likely to have sustained viral suppression (weighted odds ratio 1.69, 95% CI 1.24-2.31), lower mortality (weighted hazard ratio 0.08, 95% CI 0.03-0.20) and lower LTFU rates (weighted hazard ratio 0.08, 95% CI 0.02-0.31).
Conclusion: DSD models were associated with modestly higher quality of life, better viral suppression, and lower mortality and LTFU compared to the standard of care. These findings support the broader adoption of DSD models in delivering ART across HIV programs to enhance the QoL and clinical outcomes among PLHIV.
期刊介绍:
AIDS Research and Therapy publishes articles on basic science, translational, clinical, social, epidemiological, behavioral and educational sciences articles focused on the treatment and prevention of HIV/AIDS, and the search for the cure. The Journal publishes articles on novel and developing treatment strategies for AIDS as well as on the outcomes of established treatment strategies. Original research articles on animal models that form an essential part of the AIDS treatment research are also considered

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


