Abeer Sabry Safan, Isra Eltazi, Khaled Zammar, Suhail Hussain, Ahmad Muhammad, Khawaja Haroon, Mostafa Mahmoud, Osman Koç
{"title":"急性动脉卒中:溶栓治疗还是治疗?","authors":"Abeer Sabry Safan, Isra Eltazi, Khaled Zammar, Suhail Hussain, Ahmad Muhammad, Khawaja Haroon, Mostafa Mahmoud, Osman Koç","doi":"10.5339/qmj.2025.29","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The artery of Percheron (AOP) stroke is a rare cause of bilateral thalamic strokes, which may or may not involve the midbrain. Existing literature has identified four anatomical variants of thalamic blood supply, with AOP being the IIB variant that arises as a solitary arterial trunk from either posterior communicating artery. The clinical manifestations of AOP strokes are diverse, with no specific localizing signs. Typically, patients present with symptoms such as amnesia, gaze palsy, and hypersomnolence. The predominant underlying etiology is often cardioembolic, requiring management strategies that are tailored to the source of emboli with anticoagulation/antiplatelets.</p><p><strong>Clinical presentation: </strong>We report a case involving a 72-year-old female patient with AOP stroke characterized by a sudden loss of vision, followed by a decreased level of consciousness. Magnetic resonance imaging revealed bilateral thalamic infarcts sparing the midbrain. CTA (computed tomography angiography) revealed a filling defect at the origin of the Percheron artery arising from the left P1 segment. The patient was treated with intravenous thrombolysis. The stroke workup was unremarkable, with a normal thrombophilia workup, a transthoracic echo, and no arrhythmias detected on a prolonged Holter monitor. The patient was treated with aspirin, atorvastatin, and intensive physical and cognitive therapy. On follow-up, she regained her consciousness but exhibited residual impaired vertical eye movements and right-sided dysmetria.</p><p><strong>Conclusions: </strong>AOP stroke is a radiological diagnosis with no specific localizing neurological signs. A high index of suspicion is essential for timely diagnosis and management, as bilateral thalamic involvement can arise from a wide range of metabolic, infectious, and other vascular etiologies that could delay optimal management.</p>","PeriodicalId":53667,"journal":{"name":"Qatar Medical Journal","volume":"2025 1","pages":"29"},"PeriodicalIF":0.0000,"publicationDate":"2025-03-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12124466/pdf/","citationCount":"0","resultStr":"{\"title\":\"Acute artery of Percheron stroke: To treat or retreat with thrombolysis?\",\"authors\":\"Abeer Sabry Safan, Isra Eltazi, Khaled Zammar, Suhail Hussain, Ahmad Muhammad, Khawaja Haroon, Mostafa Mahmoud, Osman Koç\",\"doi\":\"10.5339/qmj.2025.29\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>The artery of Percheron (AOP) stroke is a rare cause of bilateral thalamic strokes, which may or may not involve the midbrain. Existing literature has identified four anatomical variants of thalamic blood supply, with AOP being the IIB variant that arises as a solitary arterial trunk from either posterior communicating artery. The clinical manifestations of AOP strokes are diverse, with no specific localizing signs. Typically, patients present with symptoms such as amnesia, gaze palsy, and hypersomnolence. The predominant underlying etiology is often cardioembolic, requiring management strategies that are tailored to the source of emboli with anticoagulation/antiplatelets.</p><p><strong>Clinical presentation: </strong>We report a case involving a 72-year-old female patient with AOP stroke characterized by a sudden loss of vision, followed by a decreased level of consciousness. Magnetic resonance imaging revealed bilateral thalamic infarcts sparing the midbrain. CTA (computed tomography angiography) revealed a filling defect at the origin of the Percheron artery arising from the left P1 segment. The patient was treated with intravenous thrombolysis. The stroke workup was unremarkable, with a normal thrombophilia workup, a transthoracic echo, and no arrhythmias detected on a prolonged Holter monitor. The patient was treated with aspirin, atorvastatin, and intensive physical and cognitive therapy. On follow-up, she regained her consciousness but exhibited residual impaired vertical eye movements and right-sided dysmetria.</p><p><strong>Conclusions: </strong>AOP stroke is a radiological diagnosis with no specific localizing neurological signs. A high index of suspicion is essential for timely diagnosis and management, as bilateral thalamic involvement can arise from a wide range of metabolic, infectious, and other vascular etiologies that could delay optimal management.</p>\",\"PeriodicalId\":53667,\"journal\":{\"name\":\"Qatar Medical Journal\",\"volume\":\"2025 1\",\"pages\":\"29\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2025-03-18\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12124466/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Qatar Medical Journal\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.5339/qmj.2025.29\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Qatar Medical Journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5339/qmj.2025.29","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"Medicine","Score":null,"Total":0}
Acute artery of Percheron stroke: To treat or retreat with thrombolysis?
Background: The artery of Percheron (AOP) stroke is a rare cause of bilateral thalamic strokes, which may or may not involve the midbrain. Existing literature has identified four anatomical variants of thalamic blood supply, with AOP being the IIB variant that arises as a solitary arterial trunk from either posterior communicating artery. The clinical manifestations of AOP strokes are diverse, with no specific localizing signs. Typically, patients present with symptoms such as amnesia, gaze palsy, and hypersomnolence. The predominant underlying etiology is often cardioembolic, requiring management strategies that are tailored to the source of emboli with anticoagulation/antiplatelets.
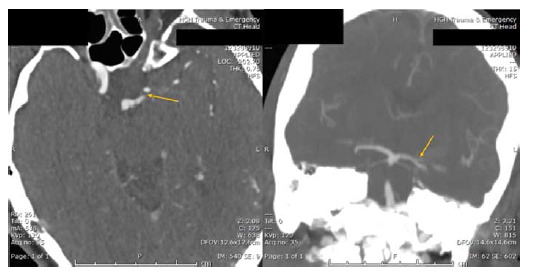
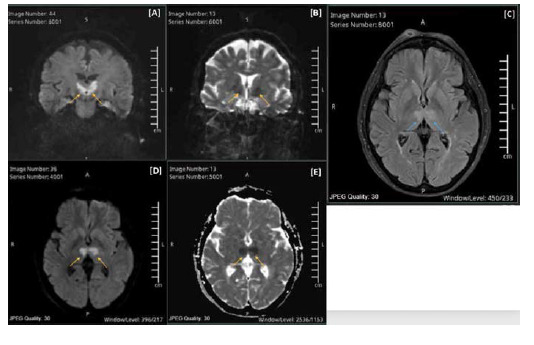
Clinical presentation: We report a case involving a 72-year-old female patient with AOP stroke characterized by a sudden loss of vision, followed by a decreased level of consciousness. Magnetic resonance imaging revealed bilateral thalamic infarcts sparing the midbrain. CTA (computed tomography angiography) revealed a filling defect at the origin of the Percheron artery arising from the left P1 segment. The patient was treated with intravenous thrombolysis. The stroke workup was unremarkable, with a normal thrombophilia workup, a transthoracic echo, and no arrhythmias detected on a prolonged Holter monitor. The patient was treated with aspirin, atorvastatin, and intensive physical and cognitive therapy. On follow-up, she regained her consciousness but exhibited residual impaired vertical eye movements and right-sided dysmetria.
Conclusions: AOP stroke is a radiological diagnosis with no specific localizing neurological signs. A high index of suspicion is essential for timely diagnosis and management, as bilateral thalamic involvement can arise from a wide range of metabolic, infectious, and other vascular etiologies that could delay optimal management.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


