Moawiah S Mustafa, George Dierking, Justin Ivoc, Glenn G Shi, Ramiro Lopez, Cole Herbel, Edward T Haupt
{"title":"全踝关节置换术术后负重CT扫描对患者体内特定器械切除的准确性。","authors":"Moawiah S Mustafa, George Dierking, Justin Ivoc, Glenn G Shi, Ramiro Lopez, Cole Herbel, Edward T Haupt","doi":"10.1177/24730114251338258","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Total ankle arthroplasty (TAA) using patient-specific instrumentation (PSI) has increased in popularity with evidence for decreased operative duration, fluoroscopy usage, and increased implant placement accuracy. To date, no comparisons have verified the accuracy of PSI in vivo using preoperative and postoperative weightbearing computed tomography (WBCT). Our study aims to supplement the literature by quantifying the accuracy and precision of PSI-guided implant positioning using WBCT. The primary study outcome is to identify positioning deviations in degrees or millimeters in any plane for talus and tibial PSI-guided resections and subsequent implant placement. Secondary outcomes were correlation and regression analyses performed to identify variables that correlate to resection or implant placement deviation, as well as comparison to existing radiography-based PSI techniques.</p><p><strong>Methods: </strong>This was a single-surgeon, single-implant consecutive patient retrospective study where preoperative and postoperative WBCTs were obtained. TAA was performed by the senior author with the same low-profile implant for all cases. Talus and tibial resection analysis was performed in computer-automated fashion on postoperative segmented WBCTs and is described as 3 possible deviations from plan (cut height in millimeters, sagittal slope, varus/valgus deviation). Overall deformity in this group was not severe. Implant placement factors independent of PSI guides are described as center-of-mass translations (mm) and axial rotation (degrees). Desired accuracy for the PSI system was within ±2 mm or ±2 degrees of the preoperative plan. Statistical analysis of data collected included Student <i>t</i> test and linear regression analyses.</p><p><strong>Results: </strong>Thirty patients were included. Four talus implants were excluded per intraoperative surgeon discretion (deviation from PSI plan, use of conventional instruments). All postoperative tibial measurements were within the desired limits, except for mediolateral center of mass positioning (<i>P</i> = .003) and slope (<i>P</i> = .013). Two of six talar parameters also diverged from preoperative measurements: axial rotation (<i>P</i> = .015) and anteroposterior positioning (<i>P</i> = .002). In addition, no correlations exceeding <i>r</i> = 0.5 were noted between preoperative deformity measurements and postoperative positioning.</p><p><strong>Conclusion: </strong>For the 26 ankles that did not require an intraoperative deviation from PSI plan and/or use of conventional instruments, total ankle replacement performed with PSI using WBCT results in component placement with relatively little deviation from the preoperative plan. In addition, the lack of correlation between preoperative deformity and implant placement suggests that the magnitude of preoperative deformity in this group was not associated with the accuracy of PSI-guided component positioning.</p><p><strong>Level of evidence: </strong>Level III, retrospective cohort study.</p>","PeriodicalId":12429,"journal":{"name":"Foot & Ankle Orthopaedics","volume":"10 2","pages":"24730114251338258"},"PeriodicalIF":0.0000,"publicationDate":"2025-05-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12123138/pdf/","citationCount":"0","resultStr":"{\"title\":\"Accuracy of Patient-Specific Instrument Resections In Vivo in Total Ankle Arthroplasty on Postoperative Weightbearing CT Scan.\",\"authors\":\"Moawiah S Mustafa, George Dierking, Justin Ivoc, Glenn G Shi, Ramiro Lopez, Cole Herbel, Edward T Haupt\",\"doi\":\"10.1177/24730114251338258\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Total ankle arthroplasty (TAA) using patient-specific instrumentation (PSI) has increased in popularity with evidence for decreased operative duration, fluoroscopy usage, and increased implant placement accuracy. To date, no comparisons have verified the accuracy of PSI in vivo using preoperative and postoperative weightbearing computed tomography (WBCT). Our study aims to supplement the literature by quantifying the accuracy and precision of PSI-guided implant positioning using WBCT. The primary study outcome is to identify positioning deviations in degrees or millimeters in any plane for talus and tibial PSI-guided resections and subsequent implant placement. Secondary outcomes were correlation and regression analyses performed to identify variables that correlate to resection or implant placement deviation, as well as comparison to existing radiography-based PSI techniques.</p><p><strong>Methods: </strong>This was a single-surgeon, single-implant consecutive patient retrospective study where preoperative and postoperative WBCTs were obtained. TAA was performed by the senior author with the same low-profile implant for all cases. Talus and tibial resection analysis was performed in computer-automated fashion on postoperative segmented WBCTs and is described as 3 possible deviations from plan (cut height in millimeters, sagittal slope, varus/valgus deviation). Overall deformity in this group was not severe. Implant placement factors independent of PSI guides are described as center-of-mass translations (mm) and axial rotation (degrees). Desired accuracy for the PSI system was within ±2 mm or ±2 degrees of the preoperative plan. Statistical analysis of data collected included Student <i>t</i> test and linear regression analyses.</p><p><strong>Results: </strong>Thirty patients were included. Four talus implants were excluded per intraoperative surgeon discretion (deviation from PSI plan, use of conventional instruments). All postoperative tibial measurements were within the desired limits, except for mediolateral center of mass positioning (<i>P</i> = .003) and slope (<i>P</i> = .013). Two of six talar parameters also diverged from preoperative measurements: axial rotation (<i>P</i> = .015) and anteroposterior positioning (<i>P</i> = .002). In addition, no correlations exceeding <i>r</i> = 0.5 were noted between preoperative deformity measurements and postoperative positioning.</p><p><strong>Conclusion: </strong>For the 26 ankles that did not require an intraoperative deviation from PSI plan and/or use of conventional instruments, total ankle replacement performed with PSI using WBCT results in component placement with relatively little deviation from the preoperative plan. In addition, the lack of correlation between preoperative deformity and implant placement suggests that the magnitude of preoperative deformity in this group was not associated with the accuracy of PSI-guided component positioning.</p><p><strong>Level of evidence: </strong>Level III, retrospective cohort study.</p>\",\"PeriodicalId\":12429,\"journal\":{\"name\":\"Foot & Ankle Orthopaedics\",\"volume\":\"10 2\",\"pages\":\"24730114251338258\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2025-05-29\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12123138/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Foot & Ankle Orthopaedics\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1177/24730114251338258\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/4/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Foot & Ankle Orthopaedics","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/24730114251338258","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/4/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
Accuracy of Patient-Specific Instrument Resections In Vivo in Total Ankle Arthroplasty on Postoperative Weightbearing CT Scan.
Background: Total ankle arthroplasty (TAA) using patient-specific instrumentation (PSI) has increased in popularity with evidence for decreased operative duration, fluoroscopy usage, and increased implant placement accuracy. To date, no comparisons have verified the accuracy of PSI in vivo using preoperative and postoperative weightbearing computed tomography (WBCT). Our study aims to supplement the literature by quantifying the accuracy and precision of PSI-guided implant positioning using WBCT. The primary study outcome is to identify positioning deviations in degrees or millimeters in any plane for talus and tibial PSI-guided resections and subsequent implant placement. Secondary outcomes were correlation and regression analyses performed to identify variables that correlate to resection or implant placement deviation, as well as comparison to existing radiography-based PSI techniques.
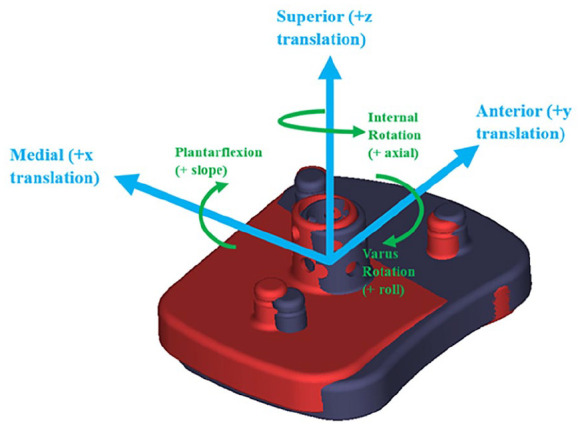
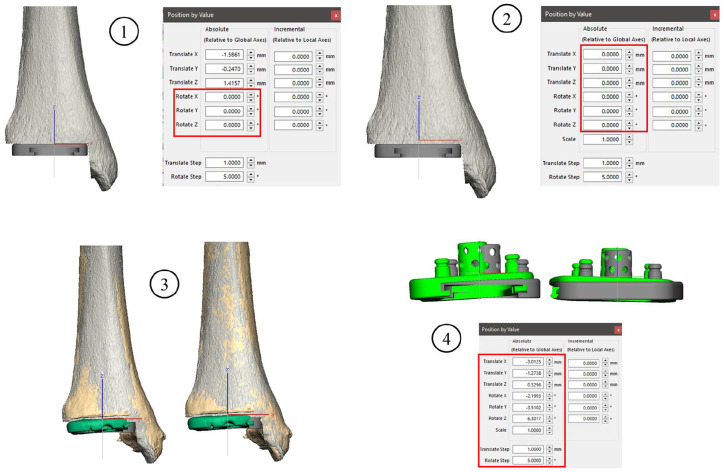
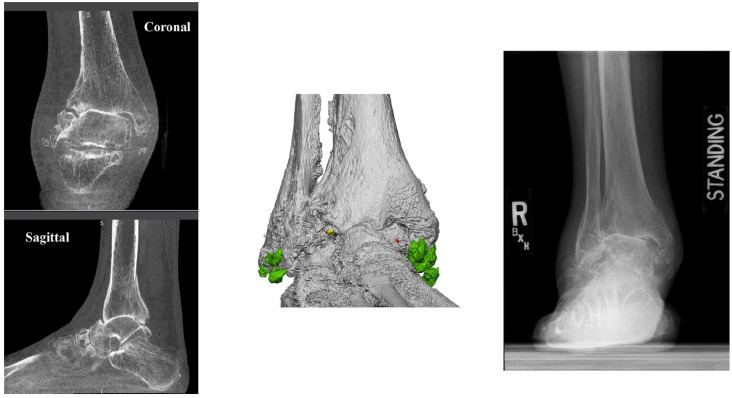
Methods: This was a single-surgeon, single-implant consecutive patient retrospective study where preoperative and postoperative WBCTs were obtained. TAA was performed by the senior author with the same low-profile implant for all cases. Talus and tibial resection analysis was performed in computer-automated fashion on postoperative segmented WBCTs and is described as 3 possible deviations from plan (cut height in millimeters, sagittal slope, varus/valgus deviation). Overall deformity in this group was not severe. Implant placement factors independent of PSI guides are described as center-of-mass translations (mm) and axial rotation (degrees). Desired accuracy for the PSI system was within ±2 mm or ±2 degrees of the preoperative plan. Statistical analysis of data collected included Student t test and linear regression analyses.
Results: Thirty patients were included. Four talus implants were excluded per intraoperative surgeon discretion (deviation from PSI plan, use of conventional instruments). All postoperative tibial measurements were within the desired limits, except for mediolateral center of mass positioning (P = .003) and slope (P = .013). Two of six talar parameters also diverged from preoperative measurements: axial rotation (P = .015) and anteroposterior positioning (P = .002). In addition, no correlations exceeding r = 0.5 were noted between preoperative deformity measurements and postoperative positioning.
Conclusion: For the 26 ankles that did not require an intraoperative deviation from PSI plan and/or use of conventional instruments, total ankle replacement performed with PSI using WBCT results in component placement with relatively little deviation from the preoperative plan. In addition, the lack of correlation between preoperative deformity and implant placement suggests that the magnitude of preoperative deformity in this group was not associated with the accuracy of PSI-guided component positioning.
Level of evidence: Level III, retrospective cohort study.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


