Azizullah Beran, Khaled Elfert, Feenalie N Patel, Mouhand Mohamed, Daryl Ramai, Almaza Albakri, Nasir Saleem, Faisal Kamal, Andrew Canakis, Khaled Srour, Danial H Shaikh, Shyam Thakkar, Douglas K Rex, Indira Bhavsar-Burke, John J Guardiola
{"title":"慢性肾脏疾病患者结肠内镜粘膜切除术后息肉切除出血的风险:美国协作网络的倾向匹配分析","authors":"Azizullah Beran, Khaled Elfert, Feenalie N Patel, Mouhand Mohamed, Daryl Ramai, Almaza Albakri, Nasir Saleem, Faisal Kamal, Andrew Canakis, Khaled Srour, Danial H Shaikh, Shyam Thakkar, Douglas K Rex, Indira Bhavsar-Burke, John J Guardiola","doi":"10.1007/s10620-025-09122-8","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Studies evaluating the risk of post-polypectomy bleeding (PPB) after colorectal endoscopic mucosal resection (EMR) in patients with chronic kidney disease (CKD) and end-stage renal disease (ESRD) are limited.</p><p><strong>Methods: </strong>This retrospective cohort study utilized the U.S. Collaborative Network to assess the risk of PPB after colorectal EMR in patients with CKD compared to controls. Using one-to-one propensity score matching (PSM), the primary outcome measured was PPB within 30 days after colorectal EMR. The PPB risk was further stratified by CKD severity: non-advanced CKD and advanced CKD.</p><p><strong>Results: </strong>After PSM, each cohort included 9,196 patients. Overall, CKD was associated with increased risk of PPB following colorectal EMR (5.4% vs. 3.8%, odds ratio [OR] 1.44, 95% confidence interval [CI] 1.25-1.66, p < 0.001). The PPB risk was significantly higher in patients with advanced CKD (8.1% vs. 4%, OR 2.09, 95% CI 1.65-2.65, p < 0.001), while those with non-advanced CKD showed modest increase in risk of PPB (4.7% vs. 4%, OR 1.20, 95% CI 1.01-1.41, p = 0.03).</p><p><strong>Conclusion: </strong>Patients with CKD had higher risk of PPB than patients without CKD. The PPB risk was notably increased in patients with advanced CKD. Optimizing patients with CKD, especially advanced CKD, before colorectal EMR and monitoring for post-procedure bleeding remains important.</p>","PeriodicalId":11378,"journal":{"name":"Digestive Diseases and Sciences","volume":" ","pages":"3102-3109"},"PeriodicalIF":2.5000,"publicationDate":"2025-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12411577/pdf/","citationCount":"0","resultStr":"{\"title\":\"Risk of Post-polypectomy Bleeding After Colorectal Endoscopic Mucosal Resection in Patients with Chronic Kidney Disease: A Propensity-Matched Analysis of the US Collaborative Network.\",\"authors\":\"Azizullah Beran, Khaled Elfert, Feenalie N Patel, Mouhand Mohamed, Daryl Ramai, Almaza Albakri, Nasir Saleem, Faisal Kamal, Andrew Canakis, Khaled Srour, Danial H Shaikh, Shyam Thakkar, Douglas K Rex, Indira Bhavsar-Burke, John J Guardiola\",\"doi\":\"10.1007/s10620-025-09122-8\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Studies evaluating the risk of post-polypectomy bleeding (PPB) after colorectal endoscopic mucosal resection (EMR) in patients with chronic kidney disease (CKD) and end-stage renal disease (ESRD) are limited.</p><p><strong>Methods: </strong>This retrospective cohort study utilized the U.S. Collaborative Network to assess the risk of PPB after colorectal EMR in patients with CKD compared to controls. Using one-to-one propensity score matching (PSM), the primary outcome measured was PPB within 30 days after colorectal EMR. The PPB risk was further stratified by CKD severity: non-advanced CKD and advanced CKD.</p><p><strong>Results: </strong>After PSM, each cohort included 9,196 patients. Overall, CKD was associated with increased risk of PPB following colorectal EMR (5.4% vs. 3.8%, odds ratio [OR] 1.44, 95% confidence interval [CI] 1.25-1.66, p < 0.001). The PPB risk was significantly higher in patients with advanced CKD (8.1% vs. 4%, OR 2.09, 95% CI 1.65-2.65, p < 0.001), while those with non-advanced CKD showed modest increase in risk of PPB (4.7% vs. 4%, OR 1.20, 95% CI 1.01-1.41, p = 0.03).</p><p><strong>Conclusion: </strong>Patients with CKD had higher risk of PPB than patients without CKD. The PPB risk was notably increased in patients with advanced CKD. Optimizing patients with CKD, especially advanced CKD, before colorectal EMR and monitoring for post-procedure bleeding remains important.</p>\",\"PeriodicalId\":11378,\"journal\":{\"name\":\"Digestive Diseases and Sciences\",\"volume\":\" \",\"pages\":\"3102-3109\"},\"PeriodicalIF\":2.5000,\"publicationDate\":\"2025-09-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12411577/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Digestive Diseases and Sciences\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s10620-025-09122-8\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/6/1 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q2\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Digestive Diseases and Sciences","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s10620-025-09122-8","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/6/1 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
背景:评估慢性肾脏疾病(CKD)和终末期肾脏疾病(ESRD)患者结肠内镜粘膜切除术(EMR)后息肉切除术后出血(PPB)风险的研究有限。方法:本回顾性队列研究利用美国协作网络来评估CKD患者结肠直肠EMR后PPB的风险,并与对照组进行比较。使用一对一倾向评分匹配(PSM),测量的主要结局是结直肠EMR后30天内的PPB。PPB风险根据CKD严重程度进一步分层:非晚期CKD和晚期CKD。结果:PSM后,每个队列包括9196例患者。总体而言,CKD与结直肠EMR后PPB风险增加相关(5.4% vs. 3.8%,优势比[OR] 1.44, 95%置信区间[CI] 1.25-1.66, p)。结论:CKD患者发生PPB的风险高于无CKD患者。晚期CKD患者发生PPB的风险显著增加。优化CKD患者,特别是晚期CKD患者,在结肠直肠EMR之前和术后出血监测仍然很重要。
Risk of Post-polypectomy Bleeding After Colorectal Endoscopic Mucosal Resection in Patients with Chronic Kidney Disease: A Propensity-Matched Analysis of the US Collaborative Network.
Background: Studies evaluating the risk of post-polypectomy bleeding (PPB) after colorectal endoscopic mucosal resection (EMR) in patients with chronic kidney disease (CKD) and end-stage renal disease (ESRD) are limited.
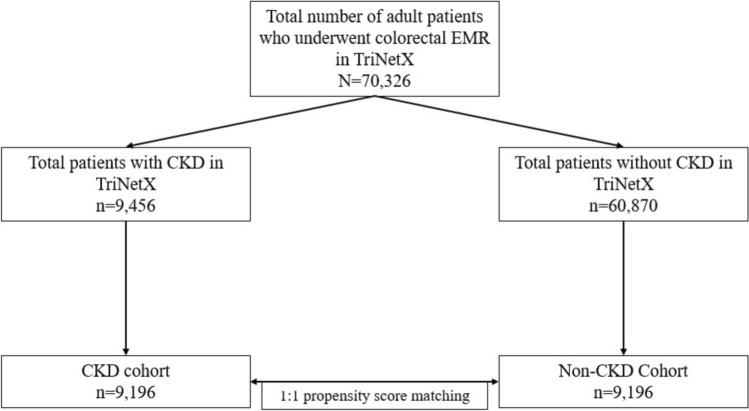
Methods: This retrospective cohort study utilized the U.S. Collaborative Network to assess the risk of PPB after colorectal EMR in patients with CKD compared to controls. Using one-to-one propensity score matching (PSM), the primary outcome measured was PPB within 30 days after colorectal EMR. The PPB risk was further stratified by CKD severity: non-advanced CKD and advanced CKD.
Results: After PSM, each cohort included 9,196 patients. Overall, CKD was associated with increased risk of PPB following colorectal EMR (5.4% vs. 3.8%, odds ratio [OR] 1.44, 95% confidence interval [CI] 1.25-1.66, p < 0.001). The PPB risk was significantly higher in patients with advanced CKD (8.1% vs. 4%, OR 2.09, 95% CI 1.65-2.65, p < 0.001), while those with non-advanced CKD showed modest increase in risk of PPB (4.7% vs. 4%, OR 1.20, 95% CI 1.01-1.41, p = 0.03).
Conclusion: Patients with CKD had higher risk of PPB than patients without CKD. The PPB risk was notably increased in patients with advanced CKD. Optimizing patients with CKD, especially advanced CKD, before colorectal EMR and monitoring for post-procedure bleeding remains important.
期刊介绍:
Digestive Diseases and Sciences publishes high-quality, peer-reviewed, original papers addressing aspects of basic/translational and clinical research in gastroenterology, hepatology, and related fields. This well-illustrated journal features comprehensive coverage of basic pathophysiology, new technological advances, and clinical breakthroughs; insights from prominent academicians and practitioners concerning new scientific developments and practical medical issues; and discussions focusing on the latest changes in local and worldwide social, economic, and governmental policies that affect the delivery of care within the disciplines of gastroenterology and hepatology.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


