Yoshiyuki Yamashita, Massimo Baudo, Serge Sicouri, Roberto Rodriguez, Eric M Gnall, Paul M Coady, Scott M Goldman, William A Gray, Basel Ramlawi
{"title":"不同血流梯度和射血分数患者经导管主动脉瓣置换术的临床效果。","authors":"Yoshiyuki Yamashita, Massimo Baudo, Serge Sicouri, Roberto Rodriguez, Eric M Gnall, Paul M Coady, Scott M Goldman, William A Gray, Basel Ramlawi","doi":"10.14744/AnatolJCardiol.2025.5157","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>To compare the clinical outcomes of transcatheter aortic valve replace-ment (TAVR) for severe aortic stenosis (AS) in patients with different flow-gradient and left ventricular ejection fraction (EF) profiles.</p><p><strong>Methods: </strong>Patients with severe AS who underwent TAVR with newer generation valves (Sapien3/3 Ultra, Evolut Pro/Pro+/FX) were retrospectively analyzed. Patients were divided into 5 groups: normal-flow high-gradient (NF-HG) AS (stroke volume index ≥ 35 mL/m2 and mean pressure gradient ≥ 40 mm Hg), low-flow high-gradient (LF-HG) with preserved EF (pEF, ≥ 50%), LF-HG with reduced EF (rEF), low-flow low-gradient (LF-LG) with pEF, and LF-LG with rEF.</p><p><strong>Results: </strong>A total of 846 patients were included in this study (NF-HG, n = 458; LF-HG with pEF, n = 142; LF-HG with rEF, n = 50; LF-LG with pEF, n = 113; LF-LG with rEF, n = 83). For the entire cohort, the median age was 82 years, and the periprocedural mortality rate was 2.1% with the highest rate in the LF-LG with rEF AS (7.2%). The 1-year and 5-year mortality rates were 13% and 51%, respectively. Multivariable Cox regression analysis showed higher all-cause mortality in the LF-HG with pEF (hazard ratio 1.42 [95% CI: 1.02-1.98]), LF-LG with pEF (1.84 [1.32-2.55]), and LF-LG with rEF (1.78 [1.22-2.61]) groups compared with the NF-HG group. Cardiovascular death rates were significantly higher in the LF-LG groups, but not in the LF-HG groups.</p><p><strong>Conclusion: </strong>In addition to both LF-LG with pEF and rEF AS, LF-HG with pEF AS had a higher all-cause mortality rate after TAVR compared to NF-HG AS.</p>","PeriodicalId":7835,"journal":{"name":"Anatolian Journal of Cardiology","volume":" ","pages":""},"PeriodicalIF":1.5000,"publicationDate":"2025-05-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12417886/pdf/","citationCount":"0","resultStr":"{\"title\":\"Clinical Outcomes of Transcatheter Aortic Valve Replacement in Patients with Various Flow-Gradient and Ejection Fraction Profiles.\",\"authors\":\"Yoshiyuki Yamashita, Massimo Baudo, Serge Sicouri, Roberto Rodriguez, Eric M Gnall, Paul M Coady, Scott M Goldman, William A Gray, Basel Ramlawi\",\"doi\":\"10.14744/AnatolJCardiol.2025.5157\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>To compare the clinical outcomes of transcatheter aortic valve replace-ment (TAVR) for severe aortic stenosis (AS) in patients with different flow-gradient and left ventricular ejection fraction (EF) profiles.</p><p><strong>Methods: </strong>Patients with severe AS who underwent TAVR with newer generation valves (Sapien3/3 Ultra, Evolut Pro/Pro+/FX) were retrospectively analyzed. Patients were divided into 5 groups: normal-flow high-gradient (NF-HG) AS (stroke volume index ≥ 35 mL/m2 and mean pressure gradient ≥ 40 mm Hg), low-flow high-gradient (LF-HG) with preserved EF (pEF, ≥ 50%), LF-HG with reduced EF (rEF), low-flow low-gradient (LF-LG) with pEF, and LF-LG with rEF.</p><p><strong>Results: </strong>A total of 846 patients were included in this study (NF-HG, n = 458; LF-HG with pEF, n = 142; LF-HG with rEF, n = 50; LF-LG with pEF, n = 113; LF-LG with rEF, n = 83). For the entire cohort, the median age was 82 years, and the periprocedural mortality rate was 2.1% with the highest rate in the LF-LG with rEF AS (7.2%). The 1-year and 5-year mortality rates were 13% and 51%, respectively. Multivariable Cox regression analysis showed higher all-cause mortality in the LF-HG with pEF (hazard ratio 1.42 [95% CI: 1.02-1.98]), LF-LG with pEF (1.84 [1.32-2.55]), and LF-LG with rEF (1.78 [1.22-2.61]) groups compared with the NF-HG group. Cardiovascular death rates were significantly higher in the LF-LG groups, but not in the LF-HG groups.</p><p><strong>Conclusion: </strong>In addition to both LF-LG with pEF and rEF AS, LF-HG with pEF AS had a higher all-cause mortality rate after TAVR compared to NF-HG AS.</p>\",\"PeriodicalId\":7835,\"journal\":{\"name\":\"Anatolian Journal of Cardiology\",\"volume\":\" \",\"pages\":\"\"},\"PeriodicalIF\":1.5000,\"publicationDate\":\"2025-05-29\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12417886/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Anatolian Journal of Cardiology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.14744/AnatolJCardiol.2025.5157\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Anatolian Journal of Cardiology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.14744/AnatolJCardiol.2025.5157","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
摘要
背景:比较不同血流梯度和左心室射血分数(EF)谱的重度主动脉瓣狭窄患者经导管主动脉瓣置换术(TAVR)的临床效果。方法:回顾性分析采用新一代瓣膜(Sapien3/3 Ultra, Evolut Pro/Pro+/FX)进行TAVR的严重AS患者。将患者分为正常流量高梯度(NF-HG) AS(脑卒中容积指数≥35 mL/m2,平均压力梯度≥40 mm Hg)、保留EF的低流量高梯度(LF-HG) (pEF≥50%)、EF减少的LF-HG (rEF)、低流量低梯度(LF-LG)合并pEF、LF-LG合并rEF 5组。结果:共纳入846例患者(NF-HG, n = 458;LF-HG伴pEF, n = 142;rEF = 50的LF-HG;带pEF的LF-LG, n = 113;LF-LG, rEF = 83)。整个队列的中位年龄为82岁,围手术期死亡率为2.1%,伴rEF AS的LF-LG患者死亡率最高(7.2%)。1年和5年死亡率分别为13%和51%。多变量Cox回归分析显示,与NF-HG组相比,LF-HG合并pEF组(风险比1.42 [95% CI: 1.02-1.98])、LF-LG合并pEF组(风险比1.84[1.32-2.55])和LF-LG合并rEF组(风险比1.78[1.22-2.61])的全因死亡率更高。心血管死亡率在LF-LG组中显著升高,但在LF-HG组中没有。结论:除了LF-LG合并pEF和rEF AS外,LF-HG合并pEF AS在TAVR后的全因死亡率高于NF-HG AS。
Clinical Outcomes of Transcatheter Aortic Valve Replacement in Patients with Various Flow-Gradient and Ejection Fraction Profiles.
Background: To compare the clinical outcomes of transcatheter aortic valve replace-ment (TAVR) for severe aortic stenosis (AS) in patients with different flow-gradient and left ventricular ejection fraction (EF) profiles.
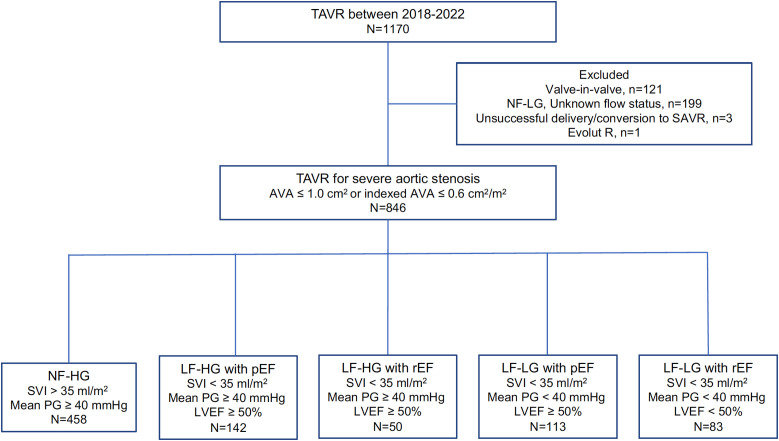
Methods: Patients with severe AS who underwent TAVR with newer generation valves (Sapien3/3 Ultra, Evolut Pro/Pro+/FX) were retrospectively analyzed. Patients were divided into 5 groups: normal-flow high-gradient (NF-HG) AS (stroke volume index ≥ 35 mL/m2 and mean pressure gradient ≥ 40 mm Hg), low-flow high-gradient (LF-HG) with preserved EF (pEF, ≥ 50%), LF-HG with reduced EF (rEF), low-flow low-gradient (LF-LG) with pEF, and LF-LG with rEF.
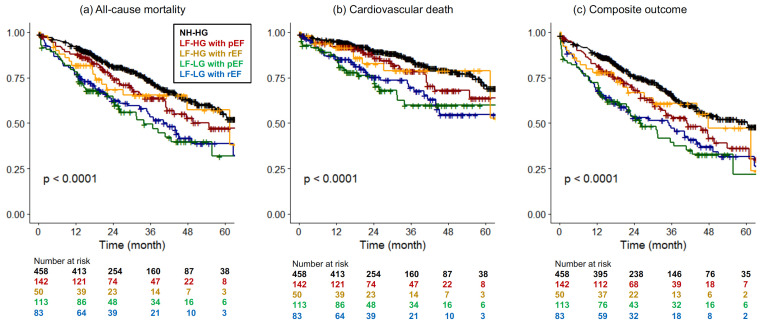
Results: A total of 846 patients were included in this study (NF-HG, n = 458; LF-HG with pEF, n = 142; LF-HG with rEF, n = 50; LF-LG with pEF, n = 113; LF-LG with rEF, n = 83). For the entire cohort, the median age was 82 years, and the periprocedural mortality rate was 2.1% with the highest rate in the LF-LG with rEF AS (7.2%). The 1-year and 5-year mortality rates were 13% and 51%, respectively. Multivariable Cox regression analysis showed higher all-cause mortality in the LF-HG with pEF (hazard ratio 1.42 [95% CI: 1.02-1.98]), LF-LG with pEF (1.84 [1.32-2.55]), and LF-LG with rEF (1.78 [1.22-2.61]) groups compared with the NF-HG group. Cardiovascular death rates were significantly higher in the LF-LG groups, but not in the LF-HG groups.
Conclusion: In addition to both LF-LG with pEF and rEF AS, LF-HG with pEF AS had a higher all-cause mortality rate after TAVR compared to NF-HG AS.
期刊介绍:
The Anatolian Journal of Cardiology is an international monthly periodical on cardiology published on independent, unbiased, double-blinded and peer-review principles. The journal’s publication language is English.
The Anatolian Journal of Cardiology aims to publish qualified and original clinical, experimental and basic research on cardiology at the international level. The journal’s scope also covers editorial comments, reviews of innovations in medical education and practice, case reports, original images, scientific letters, educational articles, letters to the editor, articles on publication ethics, diagnostic puzzles, and issues in social cardiology.
The target readership includes academic members, specialists, residents, and general practitioners working in the fields of adult cardiology, pediatric cardiology, cardiovascular surgery and internal medicine.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


