Jose Loayza Pintado, Taiwo Ajani, Daniela Hernandez, Everardo Cobos
{"title":"罕见的罪魁祸首还是伪装的难以捉摸的罪魁祸首?揭示野生型ATTR心脏淀粉样变在心力衰竭伴射血分数降低。","authors":"Jose Loayza Pintado, Taiwo Ajani, Daniela Hernandez, Everardo Cobos","doi":"10.1177/23247096251345712","DOIUrl":null,"url":null,"abstract":"<p><p>Cardiac amyloidosis (CA) is a rare disorder caused by the deposition of abnormal proteins called amyloid in the myocardium, leading to dysfunction. The 2 most common forms of amyloidosis are AL (light chain) and ATTR (transthyretin). Diagnosing amyloidosis is challenging, especially in its early stages, due to its nonspecific symptoms and overlap with other conditions. Recent studies suggest that the incidence of wild-type transthyretin amyloidosis is rising, likely due to improved diagnostic techniques and an aging population. We present the case of a 72-year-old male with lower extremity edema, progressive shortness of breath, and worsening renal function. He had a significant medical history, including hypertension, small lymphocytic lymphoma, coronary artery disease, diabetes, and chronic kidney disease. Physical examination revealed orthostatic hypotension and peripheral neuropathy. Imaging showed restrictive cardiomyopathy with reduced ejection fraction. Laboratory tests confirmed anemia and proteinuria, while a bone marrow biopsy ruled out AL amyloidosis. A Tc-99m pyrophosphate scan confirmed the diagnosis of ATTR CA. ATTR often presents with multi-organ involvement, complicating diagnosis. This patient's coexisting conditions, including orthostatic hypotension and renal failure, may have been aggravated by amyloidosis. Misdiagnosis between AL and ATTR can lead to inappropriate treatments, making accurate diagnosis crucial. ATTR requires transthyretin stabilizers and symptom management, while AL needs chemotherapy. Treatment of amyloidosis must be individualized, as autonomic dysfunction, arrhythmias, and renal involvement require careful management. Early diagnosis and differentiation are essential for appropriate treatment and improved outcomes in patients with multi-organ involvement.</p>","PeriodicalId":16198,"journal":{"name":"Journal of investigative medicine high impact case reports","volume":"13 ","pages":"23247096251345712"},"PeriodicalIF":0.8000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12126662/pdf/","citationCount":"0","resultStr":"{\"title\":\"A Rare Culprit or an Elusive Culprit in Disguise? Unraveling Wild-Type ATTR Cardiac Amyloidosis in Heart Failure With Reduced Ejection Fraction.\",\"authors\":\"Jose Loayza Pintado, Taiwo Ajani, Daniela Hernandez, Everardo Cobos\",\"doi\":\"10.1177/23247096251345712\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Cardiac amyloidosis (CA) is a rare disorder caused by the deposition of abnormal proteins called amyloid in the myocardium, leading to dysfunction. The 2 most common forms of amyloidosis are AL (light chain) and ATTR (transthyretin). Diagnosing amyloidosis is challenging, especially in its early stages, due to its nonspecific symptoms and overlap with other conditions. Recent studies suggest that the incidence of wild-type transthyretin amyloidosis is rising, likely due to improved diagnostic techniques and an aging population. We present the case of a 72-year-old male with lower extremity edema, progressive shortness of breath, and worsening renal function. He had a significant medical history, including hypertension, small lymphocytic lymphoma, coronary artery disease, diabetes, and chronic kidney disease. Physical examination revealed orthostatic hypotension and peripheral neuropathy. Imaging showed restrictive cardiomyopathy with reduced ejection fraction. Laboratory tests confirmed anemia and proteinuria, while a bone marrow biopsy ruled out AL amyloidosis. A Tc-99m pyrophosphate scan confirmed the diagnosis of ATTR CA. ATTR often presents with multi-organ involvement, complicating diagnosis. This patient's coexisting conditions, including orthostatic hypotension and renal failure, may have been aggravated by amyloidosis. Misdiagnosis between AL and ATTR can lead to inappropriate treatments, making accurate diagnosis crucial. ATTR requires transthyretin stabilizers and symptom management, while AL needs chemotherapy. Treatment of amyloidosis must be individualized, as autonomic dysfunction, arrhythmias, and renal involvement require careful management. Early diagnosis and differentiation are essential for appropriate treatment and improved outcomes in patients with multi-organ involvement.</p>\",\"PeriodicalId\":16198,\"journal\":{\"name\":\"Journal of investigative medicine high impact case reports\",\"volume\":\"13 \",\"pages\":\"23247096251345712\"},\"PeriodicalIF\":0.8000,\"publicationDate\":\"2025-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12126662/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of investigative medicine high impact case reports\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1177/23247096251345712\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/5/30 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"MEDICINE, GENERAL & INTERNAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of investigative medicine high impact case reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/23247096251345712","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/5/30 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
A Rare Culprit or an Elusive Culprit in Disguise? Unraveling Wild-Type ATTR Cardiac Amyloidosis in Heart Failure With Reduced Ejection Fraction.
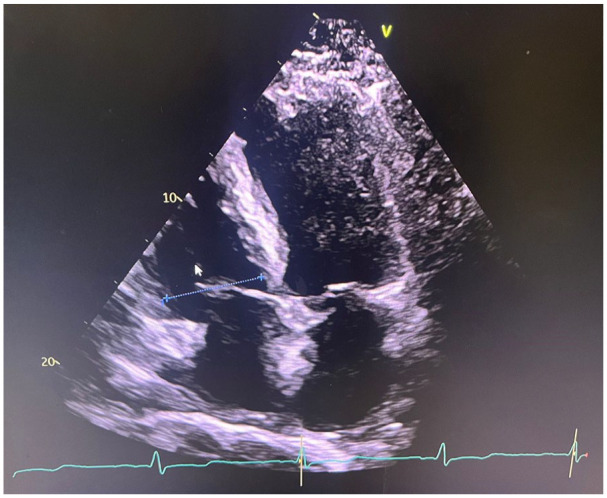
Cardiac amyloidosis (CA) is a rare disorder caused by the deposition of abnormal proteins called amyloid in the myocardium, leading to dysfunction. The 2 most common forms of amyloidosis are AL (light chain) and ATTR (transthyretin). Diagnosing amyloidosis is challenging, especially in its early stages, due to its nonspecific symptoms and overlap with other conditions. Recent studies suggest that the incidence of wild-type transthyretin amyloidosis is rising, likely due to improved diagnostic techniques and an aging population. We present the case of a 72-year-old male with lower extremity edema, progressive shortness of breath, and worsening renal function. He had a significant medical history, including hypertension, small lymphocytic lymphoma, coronary artery disease, diabetes, and chronic kidney disease. Physical examination revealed orthostatic hypotension and peripheral neuropathy. Imaging showed restrictive cardiomyopathy with reduced ejection fraction. Laboratory tests confirmed anemia and proteinuria, while a bone marrow biopsy ruled out AL amyloidosis. A Tc-99m pyrophosphate scan confirmed the diagnosis of ATTR CA. ATTR often presents with multi-organ involvement, complicating diagnosis. This patient's coexisting conditions, including orthostatic hypotension and renal failure, may have been aggravated by amyloidosis. Misdiagnosis between AL and ATTR can lead to inappropriate treatments, making accurate diagnosis crucial. ATTR requires transthyretin stabilizers and symptom management, while AL needs chemotherapy. Treatment of amyloidosis must be individualized, as autonomic dysfunction, arrhythmias, and renal involvement require careful management. Early diagnosis and differentiation are essential for appropriate treatment and improved outcomes in patients with multi-organ involvement.
期刊介绍:
The AFMR is committed to enhancing the training and career development of our members and to furthering its mission to facilitate the conduct of research to improve medical care. Case reports represent an important avenue for trainees (interns, residents, and fellows) and early-stage faculty to demonstrate productive, scholarly activity.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


