Nicole F O'Brien, Taty Tshimanga, Florette Yumsa Mangwangu, Ludovic Mayindombe, Robert Tandjeka Ekandji, Jean Pongo Mbaka, Tusekile Phiri, Sylvester June, Montfort Bernard Gushu, Hunter Wynkoop, Marlina Lovett
{"title":"脑休克指数:林德加比值在检测脑型疟疾患儿脑灌注不足中的应用。","authors":"Nicole F O'Brien, Taty Tshimanga, Florette Yumsa Mangwangu, Ludovic Mayindombe, Robert Tandjeka Ekandji, Jean Pongo Mbaka, Tusekile Phiri, Sylvester June, Montfort Bernard Gushu, Hunter Wynkoop, Marlina Lovett","doi":"10.1186/s13089-025-00430-8","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Transcranial doppler ultrasound (TCD) allows for the assessment of the cerebrovascular hemodynamics in critically ill children. Given the increasing availability of machines equipped with TCD capabilities globally, it may be a useful approach to detect cerebral hypoperfusion and guide neurologic resuscitation for pediatric patients in resource limited settings where other neuromonitoring techniques are unavailable. However, the current need to evaluate waveform characteristics and to age correct values to determine if a study is abnormal decreases the feasibility of using point of care TCD in this way. The brain shock index (BSI), a repurposing of the Lindegaard Ratio, overcomes these limitations.</p><p><strong>Methods: </strong>We performed a prospective study of children with cerebral malaria (CM). On admission and daily thereafter, TCD was used to evaluate the middle cerebral (MCA) and extra-cranial carotid arteries (Ex-ICA), and the BSI was calculated bilaterally (MCA mean flow velocity ((Vm))/Ex-ICA Vm). Neurologic outcome at discharge was assessed.</p><p><strong>Results: </strong>A cohort of 291 children with CM were evaluated. BSI calculation was successful in all of them. The mean time to perform TCD and calculate the BSI was 4 ± 2 min. Overall, 222 participants (76%) had a good outcome and 69 (24%) a poor outcome. The BSI had an AUC of 0.98 (95% CI 0.97-0.99, p < 0.0001) to predict death or moderate to severe disability. The highest sensitivity and specificity of the BSI to predict adverse outcomes occurred at a cut off value ≤ 1.1. The adjusted odds ratio of poor outcome was 3.2 (95% CI 1.6-6.1, p = 0.001) if any BSI measurement during hospitalization fell below this threshold. No intracranial pressure monitoring was available to determine the relationship between the BSIs and an invasively measured cerebral perfusion pressure.</p><p><strong>Conclusion: </strong>The BSI is a rapid, feasible point of care ultrasound measurement of cerebral hypoperfusion, with values ≤ 1.1 strongly correlating with poor neurologic outcomes in children with CM. Future studies should be performed to assess the utility of BSI to detect the presence and measure the severity of reduced cerebral perfusion pressure in other populations of critically ill children.</p>","PeriodicalId":36911,"journal":{"name":"Ultrasound Journal","volume":"17 1","pages":"27"},"PeriodicalIF":2.9000,"publicationDate":"2025-05-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12125453/pdf/","citationCount":"0","resultStr":"{\"title\":\"The brain shock index: repurposing the Lindegaard ratio for detecting cerebral hypoperfusion in children with cerebral malaria.\",\"authors\":\"Nicole F O'Brien, Taty Tshimanga, Florette Yumsa Mangwangu, Ludovic Mayindombe, Robert Tandjeka Ekandji, Jean Pongo Mbaka, Tusekile Phiri, Sylvester June, Montfort Bernard Gushu, Hunter Wynkoop, Marlina Lovett\",\"doi\":\"10.1186/s13089-025-00430-8\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Transcranial doppler ultrasound (TCD) allows for the assessment of the cerebrovascular hemodynamics in critically ill children. Given the increasing availability of machines equipped with TCD capabilities globally, it may be a useful approach to detect cerebral hypoperfusion and guide neurologic resuscitation for pediatric patients in resource limited settings where other neuromonitoring techniques are unavailable. However, the current need to evaluate waveform characteristics and to age correct values to determine if a study is abnormal decreases the feasibility of using point of care TCD in this way. The brain shock index (BSI), a repurposing of the Lindegaard Ratio, overcomes these limitations.</p><p><strong>Methods: </strong>We performed a prospective study of children with cerebral malaria (CM). On admission and daily thereafter, TCD was used to evaluate the middle cerebral (MCA) and extra-cranial carotid arteries (Ex-ICA), and the BSI was calculated bilaterally (MCA mean flow velocity ((Vm))/Ex-ICA Vm). Neurologic outcome at discharge was assessed.</p><p><strong>Results: </strong>A cohort of 291 children with CM were evaluated. BSI calculation was successful in all of them. The mean time to perform TCD and calculate the BSI was 4 ± 2 min. Overall, 222 participants (76%) had a good outcome and 69 (24%) a poor outcome. The BSI had an AUC of 0.98 (95% CI 0.97-0.99, p < 0.0001) to predict death or moderate to severe disability. The highest sensitivity and specificity of the BSI to predict adverse outcomes occurred at a cut off value ≤ 1.1. The adjusted odds ratio of poor outcome was 3.2 (95% CI 1.6-6.1, p = 0.001) if any BSI measurement during hospitalization fell below this threshold. No intracranial pressure monitoring was available to determine the relationship between the BSIs and an invasively measured cerebral perfusion pressure.</p><p><strong>Conclusion: </strong>The BSI is a rapid, feasible point of care ultrasound measurement of cerebral hypoperfusion, with values ≤ 1.1 strongly correlating with poor neurologic outcomes in children with CM. Future studies should be performed to assess the utility of BSI to detect the presence and measure the severity of reduced cerebral perfusion pressure in other populations of critically ill children.</p>\",\"PeriodicalId\":36911,\"journal\":{\"name\":\"Ultrasound Journal\",\"volume\":\"17 1\",\"pages\":\"27\"},\"PeriodicalIF\":2.9000,\"publicationDate\":\"2025-05-30\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12125453/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Ultrasound Journal\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/s13089-025-00430-8\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Ultrasound Journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s13089-025-00430-8","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
摘要
背景:经颅多普勒超声(TCD)可以评估危重儿童的脑血管血流动力学。鉴于全球配备TCD功能的机器越来越多,它可能是一种有用的方法来检测脑灌注不足,并指导小儿患者在资源有限的环境中进行神经系统复苏,而其他神经监测技术是不可用的。然而,目前需要评估波形特征和年龄正确的值来确定研究是否异常,这降低了以这种方式使用护理点TCD的可行性。脑休克指数(BSI)是对林德加德比率的重新定义,克服了这些局限性。方法:对脑型疟疾(CM)患儿进行前瞻性研究。入院时及此后每日采用TCD评估大脑中动脉(MCA)和颅外颈动脉(Ex-ICA),计算双侧BSI (MCA平均流速(Vm) /Ex-ICA Vm)。评估出院时的神经预后。结果:对291例CM患儿进行了队列评估。BSI计算均成功。执行TCD和计算BSI的平均时间为4±2分钟。总体而言,222名参与者(76%)的结果良好,69名(24%)的结果较差。BSI的AUC为0.98 (95% CI 0.97-0.99, p)。结论:BSI是一种快速、可行的脑灌注不足的护理点超声测量方法,其值≤1.1与CM患儿神经系统预后不良密切相关。未来的研究应该评估BSI在其他危重儿童人群中检测脑灌注压降低的存在和测量其严重程度的效用。
The brain shock index: repurposing the Lindegaard ratio for detecting cerebral hypoperfusion in children with cerebral malaria.
Background: Transcranial doppler ultrasound (TCD) allows for the assessment of the cerebrovascular hemodynamics in critically ill children. Given the increasing availability of machines equipped with TCD capabilities globally, it may be a useful approach to detect cerebral hypoperfusion and guide neurologic resuscitation for pediatric patients in resource limited settings where other neuromonitoring techniques are unavailable. However, the current need to evaluate waveform characteristics and to age correct values to determine if a study is abnormal decreases the feasibility of using point of care TCD in this way. The brain shock index (BSI), a repurposing of the Lindegaard Ratio, overcomes these limitations.
Methods: We performed a prospective study of children with cerebral malaria (CM). On admission and daily thereafter, TCD was used to evaluate the middle cerebral (MCA) and extra-cranial carotid arteries (Ex-ICA), and the BSI was calculated bilaterally (MCA mean flow velocity ((Vm))/Ex-ICA Vm). Neurologic outcome at discharge was assessed.
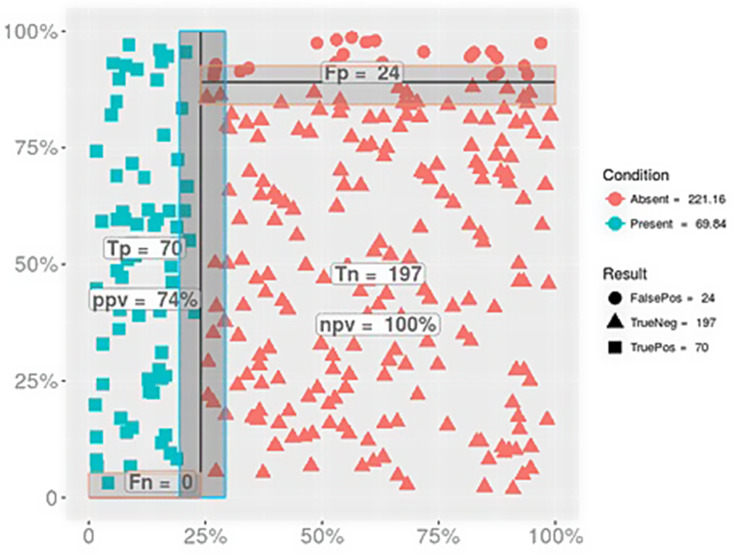
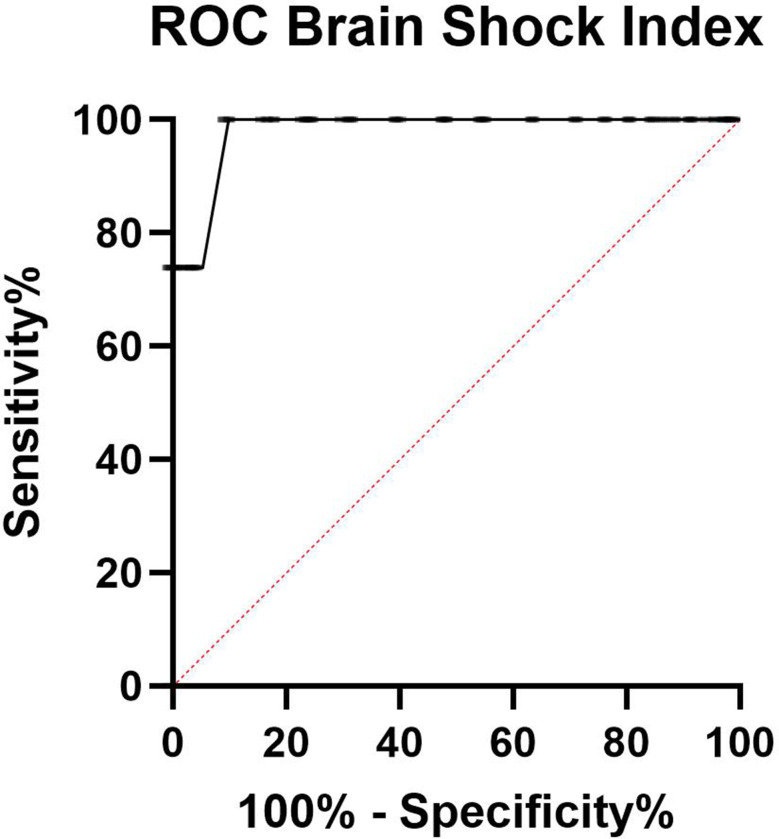
Results: A cohort of 291 children with CM were evaluated. BSI calculation was successful in all of them. The mean time to perform TCD and calculate the BSI was 4 ± 2 min. Overall, 222 participants (76%) had a good outcome and 69 (24%) a poor outcome. The BSI had an AUC of 0.98 (95% CI 0.97-0.99, p < 0.0001) to predict death or moderate to severe disability. The highest sensitivity and specificity of the BSI to predict adverse outcomes occurred at a cut off value ≤ 1.1. The adjusted odds ratio of poor outcome was 3.2 (95% CI 1.6-6.1, p = 0.001) if any BSI measurement during hospitalization fell below this threshold. No intracranial pressure monitoring was available to determine the relationship between the BSIs and an invasively measured cerebral perfusion pressure.
Conclusion: The BSI is a rapid, feasible point of care ultrasound measurement of cerebral hypoperfusion, with values ≤ 1.1 strongly correlating with poor neurologic outcomes in children with CM. Future studies should be performed to assess the utility of BSI to detect the presence and measure the severity of reduced cerebral perfusion pressure in other populations of critically ill children.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


