{"title":"增强抗利尿激素缺乏症的诊断工具:来自单中心队列研究的见解。","authors":"Alessandro Mondin, Giulia Bovo, Giorgia Antonelli, Diego Faggian, Pierluigi Mazzeo, Alessandro Bavaresco, Filippo Ceccato, Mattia Barbot","doi":"10.1007/s11102-025-01538-9","DOIUrl":null,"url":null,"abstract":"<p><strong>Context: </strong>A recent multicenter trial confirmed that hypertonic saline-stimulated copeptin is superior to the arginine stimulation test (AST) for diagnosing vasopressin deficiency (AVP-D). The latter, though less accurate, is cheaper, better tolerated, and easier to perform. We aimed to improve AST diagnostic accuracy by incorporating additional parameters alongside copeptin.</p><p><strong>Methods: </strong>We retrospectively analysed ASTs from patients evaluated for suspected AVP-D. Final diagnosis was defined based on clinical, biochemical, radiological and follow-up data. We evaluated the test diagnostic accuracy based on either literature reported or ROC-based thresholds of several variables even in combination.</p><p><strong>Results: </strong>Nineteen patients were included and 8 were diagnosed with AVP-D. Copeptin response to AST was flat in AVP-D compared to primary polydipsia (PP) but showed limited discriminatory power with the maximal accuracy for copeptin-based parameters reaching 73.7%. AVP-D patients had lower urinary osmolarity (UOsm) and higher plasma osmolarity and serum sodium (Na) at AST end. Na at AST end was the best predictor of AVP-D (≥ 141 mmol/L: sensitivity 87.5%, specificity 100%, accuracy 94.7%, AUC 0.989). A multistep approach initially assessing Na at AST end and, in dubious cases (140-142 mmol/l), also either copeptin peak (≤ 4.1 pmol/L), UOsm (≤ 428 mOsm/kg), or absent posterior pituitary hyperintense signal achieved 100% diagnostic accuracy. Logistic regression using Na at AST end values combined with any of these aforementioned additional variables also reached complete discrimination between AVP-D and PP.</p><p><strong>Discussion: </strong>Combining multiple parameters after AST improved diagnostic accuracy, even without measuring copeptin. Despite the study's retrospective design, small sample, and absence of hypertonic saline testing, findings support the potential utility of a multivariable approach to AST interpretation.</p>","PeriodicalId":20202,"journal":{"name":"Pituitary","volume":"28 3","pages":"65"},"PeriodicalIF":3.4000,"publicationDate":"2025-05-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12122565/pdf/","citationCount":"0","resultStr":"{\"title\":\"Enhancing diagnostic tools for vasopressin deficiency: insights from a single-center cohort study.\",\"authors\":\"Alessandro Mondin, Giulia Bovo, Giorgia Antonelli, Diego Faggian, Pierluigi Mazzeo, Alessandro Bavaresco, Filippo Ceccato, Mattia Barbot\",\"doi\":\"10.1007/s11102-025-01538-9\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Context: </strong>A recent multicenter trial confirmed that hypertonic saline-stimulated copeptin is superior to the arginine stimulation test (AST) for diagnosing vasopressin deficiency (AVP-D). The latter, though less accurate, is cheaper, better tolerated, and easier to perform. We aimed to improve AST diagnostic accuracy by incorporating additional parameters alongside copeptin.</p><p><strong>Methods: </strong>We retrospectively analysed ASTs from patients evaluated for suspected AVP-D. Final diagnosis was defined based on clinical, biochemical, radiological and follow-up data. We evaluated the test diagnostic accuracy based on either literature reported or ROC-based thresholds of several variables even in combination.</p><p><strong>Results: </strong>Nineteen patients were included and 8 were diagnosed with AVP-D. Copeptin response to AST was flat in AVP-D compared to primary polydipsia (PP) but showed limited discriminatory power with the maximal accuracy for copeptin-based parameters reaching 73.7%. AVP-D patients had lower urinary osmolarity (UOsm) and higher plasma osmolarity and serum sodium (Na) at AST end. Na at AST end was the best predictor of AVP-D (≥ 141 mmol/L: sensitivity 87.5%, specificity 100%, accuracy 94.7%, AUC 0.989). A multistep approach initially assessing Na at AST end and, in dubious cases (140-142 mmol/l), also either copeptin peak (≤ 4.1 pmol/L), UOsm (≤ 428 mOsm/kg), or absent posterior pituitary hyperintense signal achieved 100% diagnostic accuracy. Logistic regression using Na at AST end values combined with any of these aforementioned additional variables also reached complete discrimination between AVP-D and PP.</p><p><strong>Discussion: </strong>Combining multiple parameters after AST improved diagnostic accuracy, even without measuring copeptin. Despite the study's retrospective design, small sample, and absence of hypertonic saline testing, findings support the potential utility of a multivariable approach to AST interpretation.</p>\",\"PeriodicalId\":20202,\"journal\":{\"name\":\"Pituitary\",\"volume\":\"28 3\",\"pages\":\"65\"},\"PeriodicalIF\":3.4000,\"publicationDate\":\"2025-05-29\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12122565/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Pituitary\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s11102-025-01538-9\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"ENDOCRINOLOGY & METABOLISM\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pituitary","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s11102-025-01538-9","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
Enhancing diagnostic tools for vasopressin deficiency: insights from a single-center cohort study.
Context: A recent multicenter trial confirmed that hypertonic saline-stimulated copeptin is superior to the arginine stimulation test (AST) for diagnosing vasopressin deficiency (AVP-D). The latter, though less accurate, is cheaper, better tolerated, and easier to perform. We aimed to improve AST diagnostic accuracy by incorporating additional parameters alongside copeptin.
Methods: We retrospectively analysed ASTs from patients evaluated for suspected AVP-D. Final diagnosis was defined based on clinical, biochemical, radiological and follow-up data. We evaluated the test diagnostic accuracy based on either literature reported or ROC-based thresholds of several variables even in combination.
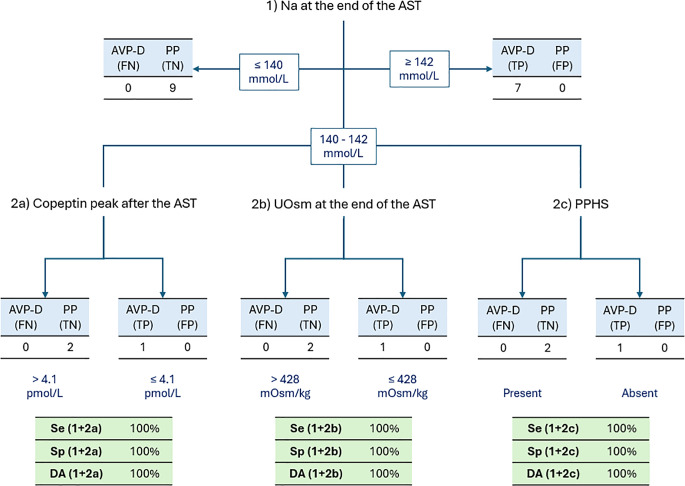
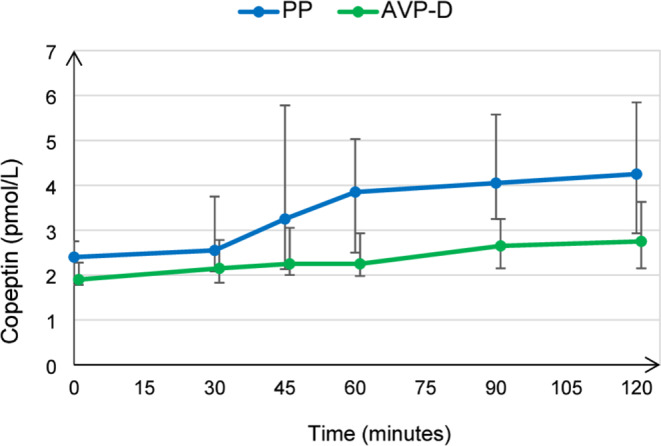
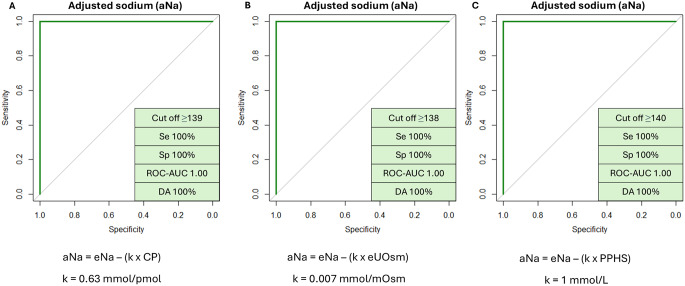
Results: Nineteen patients were included and 8 were diagnosed with AVP-D. Copeptin response to AST was flat in AVP-D compared to primary polydipsia (PP) but showed limited discriminatory power with the maximal accuracy for copeptin-based parameters reaching 73.7%. AVP-D patients had lower urinary osmolarity (UOsm) and higher plasma osmolarity and serum sodium (Na) at AST end. Na at AST end was the best predictor of AVP-D (≥ 141 mmol/L: sensitivity 87.5%, specificity 100%, accuracy 94.7%, AUC 0.989). A multistep approach initially assessing Na at AST end and, in dubious cases (140-142 mmol/l), also either copeptin peak (≤ 4.1 pmol/L), UOsm (≤ 428 mOsm/kg), or absent posterior pituitary hyperintense signal achieved 100% diagnostic accuracy. Logistic regression using Na at AST end values combined with any of these aforementioned additional variables also reached complete discrimination between AVP-D and PP.
Discussion: Combining multiple parameters after AST improved diagnostic accuracy, even without measuring copeptin. Despite the study's retrospective design, small sample, and absence of hypertonic saline testing, findings support the potential utility of a multivariable approach to AST interpretation.
期刊介绍:
Pituitary is an international publication devoted to basic and clinical aspects of the pituitary gland. It is designed to publish original, high quality research in both basic and pituitary function as well as clinical pituitary disease.
The journal considers:
Biology of Pituitary Tumors
Mechanisms of Pituitary Hormone Secretion
Regulation of Pituitary Function
Prospective Clinical Studies of Pituitary Disease
Critical Basic and Clinical Reviews
Pituitary is directed at basic investigators, physiologists, clinical adult and pediatric endocrinologists, neurosurgeons and reproductive endocrinologists interested in the broad field of the pituitary and its disorders. The Editorial Board has been drawn from international experts in basic and clinical endocrinology. The journal offers a rapid turnaround time for review of manuscripts, and the high standard of the journal is maintained by a selective peer-review process which aims to publish only the highest quality manuscripts. Pituitary will foster the publication of creative scholarship as it pertains to the pituitary and will provide a forum for basic scientists and clinicians to publish their high quality pituitary-related work.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


