{"title":"埃塞俄比亚亚的斯亚贝巴选定政府医院1型糖尿病儿童糖尿病酮症酸中毒恢复时间及其预测因素一项为期五年的回顾性随访研究。","authors":"Shimeles Tefera Mamo, Tigistu Gebreyohannis Gebretensaye, Feven Mulugeta, Gemechu Gelan Bekele","doi":"10.1177/20503121251343175","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Diabetic ketoacidosis, a severe complication of type 1 diabetes, remains a major cause of morbidity and mortality in children, particularly in resource-limited settings such as Ethiopia. Despite its high burden, data on recovery time and predictors of diabetic ketoacidosis in this population are scarce. Therefore, this study aimed to assess the time to recovery from diabetic ketoacidosis and its predictors among children with diabetic ketoacidosis at selected governmental hospitals in Addis Ababa, Ethiopia.</p><p><strong>Methods: </strong>A 5-year retrospective follow-up study was conducted among 391 hospitalized children with diabetic ketoacidosis in selected governmental hospitals in Addis Ababa, from January 1, 2018 to December 30, 2022. Participants and hospitals were selected using a simple random sampling method. A structured data collection checklist was adapted from similar studies and modified. The data were checked for completeness and entered into Stata version 16 for analysis. Variables with <i>p</i>-value < 0.05 in the multivariate Cox proportional hazards model were considered significant predictors of the time to recovery from diabetic ketoacidosis.</p><p><strong>Results: </strong>A total of 423 records of children with diabetic ketoacidosis with 391 (92.4%) response rates were included in the final analysis. Out of these, 370 were recovered and discharged. The remaining 21 cases were censored. The overall median time taken to resolution from diabetic ketoacidosis was 27 h, with an interquartile range of 16-38. Diabetic mellitus history (Adjusted Hazard Ratio (AHR) = 0.41, 95% CI: 0.30-0.56), severity of diabetic ketoacidosis (AHR = 2.35, 95% CI: 1.34-6.1), presence of comorbidity (AHR = 1.76, 95% CI: 1.37-2.26), and blood sugar level (AHR = 0.61, 95% CI: 0.39-0.96) were all independent predictors of time to recovery from diabetic ketoacidosis.</p><p><strong>Conclusion and recommendation: </strong>The median diabetic ketoacidosis recovery time was 27 h. Key predictors included admission glucose, comorbidities, diabetic ketoacidosis severity, and diabetes history. Early diagnosis, thorough assessment, and optimized management are crucial to reducing risks and improving outcomes.</p>","PeriodicalId":21398,"journal":{"name":"SAGE Open Medicine","volume":"13 ","pages":"20503121251343175"},"PeriodicalIF":2.1000,"publicationDate":"2025-05-26","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12106986/pdf/","citationCount":"0","resultStr":"{\"title\":\"Time to recovery from diabetic ketoacidosis and its predictors among children with type 1 diabetes at selected governmental hospitals in Addis Ababa, Ethiopia; A five-year retrospective follow-up study.\",\"authors\":\"Shimeles Tefera Mamo, Tigistu Gebreyohannis Gebretensaye, Feven Mulugeta, Gemechu Gelan Bekele\",\"doi\":\"10.1177/20503121251343175\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Diabetic ketoacidosis, a severe complication of type 1 diabetes, remains a major cause of morbidity and mortality in children, particularly in resource-limited settings such as Ethiopia. Despite its high burden, data on recovery time and predictors of diabetic ketoacidosis in this population are scarce. Therefore, this study aimed to assess the time to recovery from diabetic ketoacidosis and its predictors among children with diabetic ketoacidosis at selected governmental hospitals in Addis Ababa, Ethiopia.</p><p><strong>Methods: </strong>A 5-year retrospective follow-up study was conducted among 391 hospitalized children with diabetic ketoacidosis in selected governmental hospitals in Addis Ababa, from January 1, 2018 to December 30, 2022. Participants and hospitals were selected using a simple random sampling method. A structured data collection checklist was adapted from similar studies and modified. The data were checked for completeness and entered into Stata version 16 for analysis. Variables with <i>p</i>-value < 0.05 in the multivariate Cox proportional hazards model were considered significant predictors of the time to recovery from diabetic ketoacidosis.</p><p><strong>Results: </strong>A total of 423 records of children with diabetic ketoacidosis with 391 (92.4%) response rates were included in the final analysis. Out of these, 370 were recovered and discharged. The remaining 21 cases were censored. The overall median time taken to resolution from diabetic ketoacidosis was 27 h, with an interquartile range of 16-38. Diabetic mellitus history (Adjusted Hazard Ratio (AHR) = 0.41, 95% CI: 0.30-0.56), severity of diabetic ketoacidosis (AHR = 2.35, 95% CI: 1.34-6.1), presence of comorbidity (AHR = 1.76, 95% CI: 1.37-2.26), and blood sugar level (AHR = 0.61, 95% CI: 0.39-0.96) were all independent predictors of time to recovery from diabetic ketoacidosis.</p><p><strong>Conclusion and recommendation: </strong>The median diabetic ketoacidosis recovery time was 27 h. Key predictors included admission glucose, comorbidities, diabetic ketoacidosis severity, and diabetes history. Early diagnosis, thorough assessment, and optimized management are crucial to reducing risks and improving outcomes.</p>\",\"PeriodicalId\":21398,\"journal\":{\"name\":\"SAGE Open Medicine\",\"volume\":\"13 \",\"pages\":\"20503121251343175\"},\"PeriodicalIF\":2.1000,\"publicationDate\":\"2025-05-26\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12106986/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"SAGE Open Medicine\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1177/20503121251343175\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"MEDICINE, GENERAL & INTERNAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"SAGE Open Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/20503121251343175","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
Time to recovery from diabetic ketoacidosis and its predictors among children with type 1 diabetes at selected governmental hospitals in Addis Ababa, Ethiopia; A five-year retrospective follow-up study.
Background: Diabetic ketoacidosis, a severe complication of type 1 diabetes, remains a major cause of morbidity and mortality in children, particularly in resource-limited settings such as Ethiopia. Despite its high burden, data on recovery time and predictors of diabetic ketoacidosis in this population are scarce. Therefore, this study aimed to assess the time to recovery from diabetic ketoacidosis and its predictors among children with diabetic ketoacidosis at selected governmental hospitals in Addis Ababa, Ethiopia.
Methods: A 5-year retrospective follow-up study was conducted among 391 hospitalized children with diabetic ketoacidosis in selected governmental hospitals in Addis Ababa, from January 1, 2018 to December 30, 2022. Participants and hospitals were selected using a simple random sampling method. A structured data collection checklist was adapted from similar studies and modified. The data were checked for completeness and entered into Stata version 16 for analysis. Variables with p-value < 0.05 in the multivariate Cox proportional hazards model were considered significant predictors of the time to recovery from diabetic ketoacidosis.
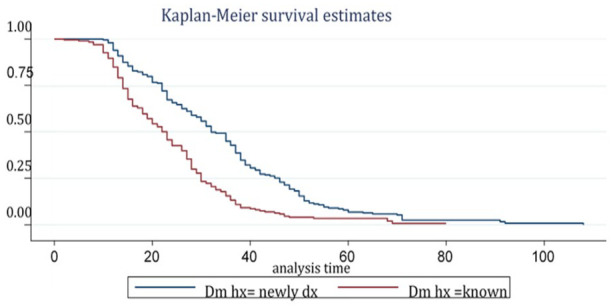
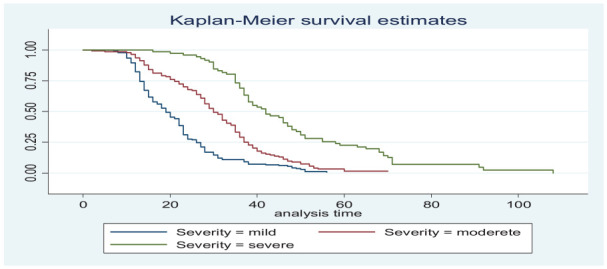
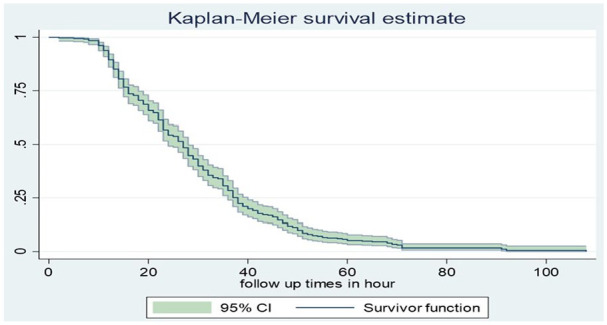
Results: A total of 423 records of children with diabetic ketoacidosis with 391 (92.4%) response rates were included in the final analysis. Out of these, 370 were recovered and discharged. The remaining 21 cases were censored. The overall median time taken to resolution from diabetic ketoacidosis was 27 h, with an interquartile range of 16-38. Diabetic mellitus history (Adjusted Hazard Ratio (AHR) = 0.41, 95% CI: 0.30-0.56), severity of diabetic ketoacidosis (AHR = 2.35, 95% CI: 1.34-6.1), presence of comorbidity (AHR = 1.76, 95% CI: 1.37-2.26), and blood sugar level (AHR = 0.61, 95% CI: 0.39-0.96) were all independent predictors of time to recovery from diabetic ketoacidosis.
Conclusion and recommendation: The median diabetic ketoacidosis recovery time was 27 h. Key predictors included admission glucose, comorbidities, diabetic ketoacidosis severity, and diabetes history. Early diagnosis, thorough assessment, and optimized management are crucial to reducing risks and improving outcomes.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


