{"title":"狼疮-克鲁斯肾炎方案的长期疗效和安全性:狼疮-克鲁斯和狼疮-波尔多队列的倾向评分研究。","authors":"Guillermo Ruiz-Irastorza, Beatriz Marín-García, Luis Dueña-Bartolomé, Diana Paredes Ruiz, Amaia Osorio, Estibaliz Lazaro","doi":"10.1136/lupus-2025-001562","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>To assess the efficacy and toxicity of the Lupus-Cruces Nephritis (LCN) protocol compared with standard of care (SOC) with cyclophosphamide (CYC) or mycophenolate in patients with lupus nephritis (LN) during an extended follow-up time up to 10 years.</p><p><strong>Methods: </strong>Patients with biopsy-proven class III, IV or V LN treated with LCN were compared with SOC. Patients in the LCN were treated with a CYC plus repeated methylprednisolone pulse-based regimen. The achievement of complete renal response (CRR) and the progression to chronic kidney disease (CKD) were the two main outcomes. Glucocorticoid (GC)-related toxicity, major infections and damage accrual were also analysed. A propensity score (PS)-adjusted multivariate analysis was used to overcome the confounding-by-indication bias.</p><p><strong>Results: </strong>147 patients were included in this study (47 LCN and 100 SOC). CRR at 12 months was 85% vs 44%, respectively (p<0.001). Eventually, 96% patients in the LCN group achieved CRR vs 74% patients in the SOC (p=0.002). In the multivariate PS-adjusted Cox model, LCN patients were more likely to eventually achieve CRR (PS-adjusted HR 3.5, 95% CI 2.2 to 5.5, p<0.001). The risk of progression to CKD was lower in LCN patients (PS-adjusted HR 0.3, 95% CI 0.11 to 0.82, p=0.019). The risks of GC-induced toxicity, renal or GC-related damage accrual and major infections were also lower in the LCN group: adjusted HR 0.09, 95% CI 0.02 to 0.39; PS-adjusted HR 0.14, 95% CI 0.04 to 0.4; PS-adjusted HR 0.2, 95% CI 0.046 to 0.95; respectively.</p><p><strong>Conclusions: </strong>This study confirms the LCN protocol as an effective and safe, in addition to widely available and affordable, regimen for the induction therapy of LN.</p>","PeriodicalId":18126,"journal":{"name":"Lupus Science & Medicine","volume":"12 1","pages":""},"PeriodicalIF":3.5000,"publicationDate":"2025-05-26","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12107586/pdf/","citationCount":"0","resultStr":"{\"title\":\"Long-term efficacy and safety of the Lupus-Cruces Nephritis protocol: a propensity score study of the Lupus-Cruces and Lupus-Bordeaux cohorts.\",\"authors\":\"Guillermo Ruiz-Irastorza, Beatriz Marín-García, Luis Dueña-Bartolomé, Diana Paredes Ruiz, Amaia Osorio, Estibaliz Lazaro\",\"doi\":\"10.1136/lupus-2025-001562\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>To assess the efficacy and toxicity of the Lupus-Cruces Nephritis (LCN) protocol compared with standard of care (SOC) with cyclophosphamide (CYC) or mycophenolate in patients with lupus nephritis (LN) during an extended follow-up time up to 10 years.</p><p><strong>Methods: </strong>Patients with biopsy-proven class III, IV or V LN treated with LCN were compared with SOC. Patients in the LCN were treated with a CYC plus repeated methylprednisolone pulse-based regimen. The achievement of complete renal response (CRR) and the progression to chronic kidney disease (CKD) were the two main outcomes. Glucocorticoid (GC)-related toxicity, major infections and damage accrual were also analysed. A propensity score (PS)-adjusted multivariate analysis was used to overcome the confounding-by-indication bias.</p><p><strong>Results: </strong>147 patients were included in this study (47 LCN and 100 SOC). CRR at 12 months was 85% vs 44%, respectively (p<0.001). Eventually, 96% patients in the LCN group achieved CRR vs 74% patients in the SOC (p=0.002). In the multivariate PS-adjusted Cox model, LCN patients were more likely to eventually achieve CRR (PS-adjusted HR 3.5, 95% CI 2.2 to 5.5, p<0.001). The risk of progression to CKD was lower in LCN patients (PS-adjusted HR 0.3, 95% CI 0.11 to 0.82, p=0.019). The risks of GC-induced toxicity, renal or GC-related damage accrual and major infections were also lower in the LCN group: adjusted HR 0.09, 95% CI 0.02 to 0.39; PS-adjusted HR 0.14, 95% CI 0.04 to 0.4; PS-adjusted HR 0.2, 95% CI 0.046 to 0.95; respectively.</p><p><strong>Conclusions: </strong>This study confirms the LCN protocol as an effective and safe, in addition to widely available and affordable, regimen for the induction therapy of LN.</p>\",\"PeriodicalId\":18126,\"journal\":{\"name\":\"Lupus Science & Medicine\",\"volume\":\"12 1\",\"pages\":\"\"},\"PeriodicalIF\":3.5000,\"publicationDate\":\"2025-05-26\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12107586/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Lupus Science & Medicine\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1136/lupus-2025-001562\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"RHEUMATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Lupus Science & Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1136/lupus-2025-001562","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"RHEUMATOLOGY","Score":null,"Total":0}
Long-term efficacy and safety of the Lupus-Cruces Nephritis protocol: a propensity score study of the Lupus-Cruces and Lupus-Bordeaux cohorts.
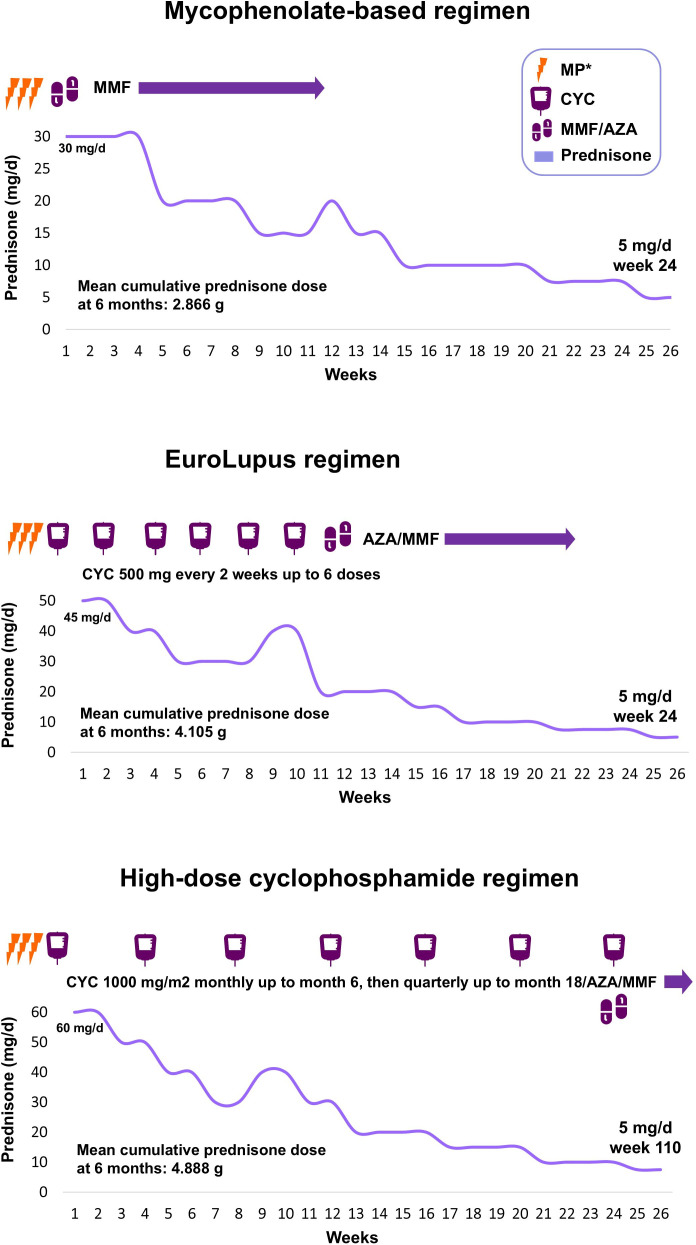
Objective: To assess the efficacy and toxicity of the Lupus-Cruces Nephritis (LCN) protocol compared with standard of care (SOC) with cyclophosphamide (CYC) or mycophenolate in patients with lupus nephritis (LN) during an extended follow-up time up to 10 years.
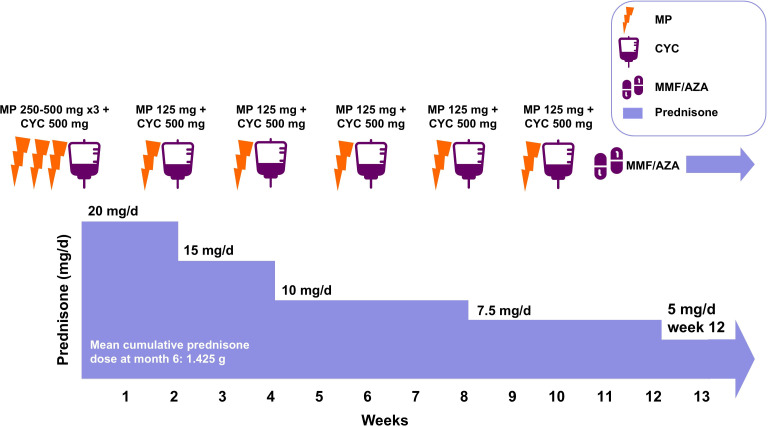
Methods: Patients with biopsy-proven class III, IV or V LN treated with LCN were compared with SOC. Patients in the LCN were treated with a CYC plus repeated methylprednisolone pulse-based regimen. The achievement of complete renal response (CRR) and the progression to chronic kidney disease (CKD) were the two main outcomes. Glucocorticoid (GC)-related toxicity, major infections and damage accrual were also analysed. A propensity score (PS)-adjusted multivariate analysis was used to overcome the confounding-by-indication bias.
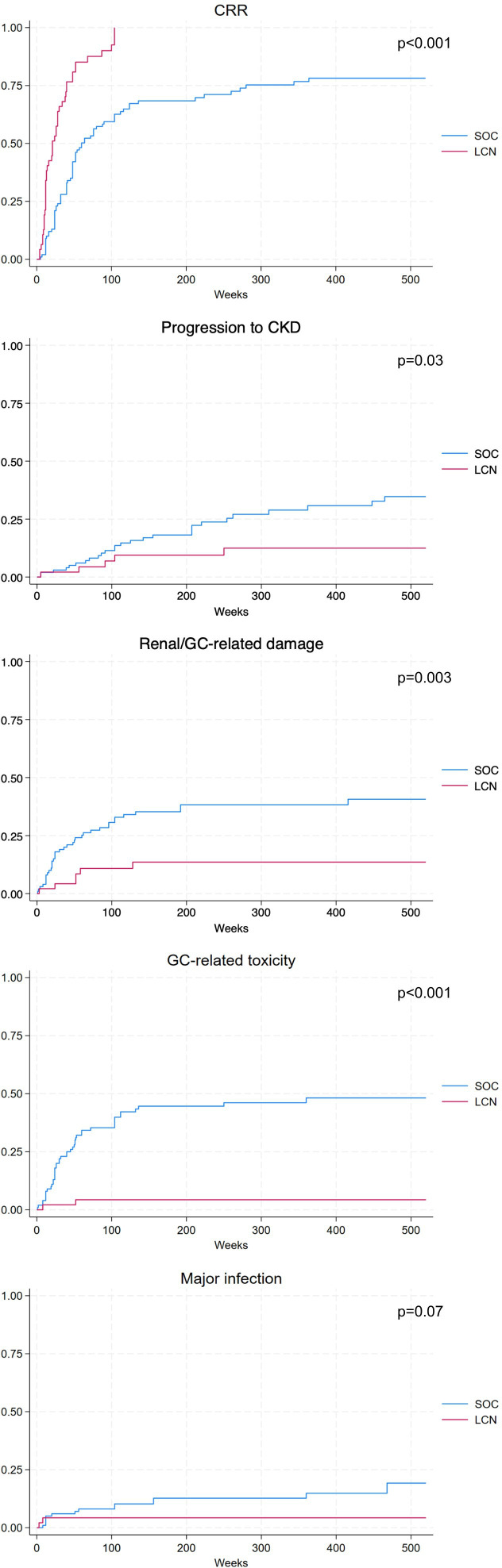
Results: 147 patients were included in this study (47 LCN and 100 SOC). CRR at 12 months was 85% vs 44%, respectively (p<0.001). Eventually, 96% patients in the LCN group achieved CRR vs 74% patients in the SOC (p=0.002). In the multivariate PS-adjusted Cox model, LCN patients were more likely to eventually achieve CRR (PS-adjusted HR 3.5, 95% CI 2.2 to 5.5, p<0.001). The risk of progression to CKD was lower in LCN patients (PS-adjusted HR 0.3, 95% CI 0.11 to 0.82, p=0.019). The risks of GC-induced toxicity, renal or GC-related damage accrual and major infections were also lower in the LCN group: adjusted HR 0.09, 95% CI 0.02 to 0.39; PS-adjusted HR 0.14, 95% CI 0.04 to 0.4; PS-adjusted HR 0.2, 95% CI 0.046 to 0.95; respectively.
Conclusions: This study confirms the LCN protocol as an effective and safe, in addition to widely available and affordable, regimen for the induction therapy of LN.
期刊介绍:
Lupus Science & Medicine is a global, peer reviewed, open access online journal that provides a central point for publication of basic, clinical, translational, and epidemiological studies of all aspects of lupus and related diseases. It is the first lupus-specific open access journal in the world and was developed in response to the need for a barrier-free forum for publication of groundbreaking studies in lupus. The journal publishes research on lupus from fields including, but not limited to: rheumatology, dermatology, nephrology, immunology, pediatrics, cardiology, hepatology, pulmonology, obstetrics and gynecology, and psychiatry.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


