Mahmoud Balata, Tetsu Tanaka, Atsushi Sugiura, Refik Kavsur, Johanna Vogelhuber, Can Öztürk, Sebastian Zimmer, Julian Luetkens, Georg Nickenig, Marcel Weber
{"title":"腰大肌面积与经导管三尖瓣修复后预后的关系。","authors":"Mahmoud Balata, Tetsu Tanaka, Atsushi Sugiura, Refik Kavsur, Johanna Vogelhuber, Can Öztürk, Sebastian Zimmer, Julian Luetkens, Georg Nickenig, Marcel Weber","doi":"10.1007/s12928-025-01136-3","DOIUrl":null,"url":null,"abstract":"<p><p>Transcatheter tricuspid valve repair (TTVR) might be an alternative option to reduce tricuspid regurgitation (TR) in patients with sarcopenia. Psoas muscle area (PMA) measured using computed tomography (CT) is known as a marker of sarcopenia. We investigated the association of PMA with procedural and clinical outcomes following TTVR. We retrospectively measured left and right PMA using pre-procedural CT in patients undergoing TTVR. Low PMA was defined as the total PMA < 20.3 cm<sup>2</sup> for men and < 11.8 cm<sup>2</sup> for women. The primary outcome was a composite of all-cause mortality and heart failure hospitalization within one year after TTVR. Of 163 patients, 47 (29%) were considered as having low PMA. Procedural success, defined as residual TR of ≤ 2 + at discharge, and in-hospital mortality were comparable between patients with low and high PMA. Patients with low PMA had a higher incidence of the composite outcome than those with high PMA (49% vs. 21%; p = 0.001) This association was consistent after adjusting for baseline characteristics (adjusted hazard ratio 0.43; 95% confidence interval: 0.23-0.80; p = 0.008). In contrast, the New York Heart Association functional class improved from baseline to three-month follow-up, regardless of PMA. Approximately 30% of patients undergoing TTVR were found to have low PMA. Although TTVR may be a safe therapeutic option to reduce TR and improve heart failure symptoms in patients with sarcopenia, the prognosis after TTVR remains poor in this population. Pre-procedural CT-based assessment of PMA may enhance risk stratification and support better clinical decision-making for TTVR.</p>","PeriodicalId":9439,"journal":{"name":"Cardiovascular Intervention and Therapeutics","volume":" ","pages":"679-688"},"PeriodicalIF":5.8000,"publicationDate":"2025-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12167307/pdf/","citationCount":"0","resultStr":"{\"title\":\"Association between psoas muscle area and outcomes after transcatheter tricuspid valve repair.\",\"authors\":\"Mahmoud Balata, Tetsu Tanaka, Atsushi Sugiura, Refik Kavsur, Johanna Vogelhuber, Can Öztürk, Sebastian Zimmer, Julian Luetkens, Georg Nickenig, Marcel Weber\",\"doi\":\"10.1007/s12928-025-01136-3\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Transcatheter tricuspid valve repair (TTVR) might be an alternative option to reduce tricuspid regurgitation (TR) in patients with sarcopenia. Psoas muscle area (PMA) measured using computed tomography (CT) is known as a marker of sarcopenia. We investigated the association of PMA with procedural and clinical outcomes following TTVR. We retrospectively measured left and right PMA using pre-procedural CT in patients undergoing TTVR. Low PMA was defined as the total PMA < 20.3 cm<sup>2</sup> for men and < 11.8 cm<sup>2</sup> for women. The primary outcome was a composite of all-cause mortality and heart failure hospitalization within one year after TTVR. Of 163 patients, 47 (29%) were considered as having low PMA. Procedural success, defined as residual TR of ≤ 2 + at discharge, and in-hospital mortality were comparable between patients with low and high PMA. Patients with low PMA had a higher incidence of the composite outcome than those with high PMA (49% vs. 21%; p = 0.001) This association was consistent after adjusting for baseline characteristics (adjusted hazard ratio 0.43; 95% confidence interval: 0.23-0.80; p = 0.008). In contrast, the New York Heart Association functional class improved from baseline to three-month follow-up, regardless of PMA. Approximately 30% of patients undergoing TTVR were found to have low PMA. Although TTVR may be a safe therapeutic option to reduce TR and improve heart failure symptoms in patients with sarcopenia, the prognosis after TTVR remains poor in this population. Pre-procedural CT-based assessment of PMA may enhance risk stratification and support better clinical decision-making for TTVR.</p>\",\"PeriodicalId\":9439,\"journal\":{\"name\":\"Cardiovascular Intervention and Therapeutics\",\"volume\":\" \",\"pages\":\"679-688\"},\"PeriodicalIF\":5.8000,\"publicationDate\":\"2025-07-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12167307/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Cardiovascular Intervention and Therapeutics\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1007/s12928-025-01136-3\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/5/27 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q2\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cardiovascular Intervention and Therapeutics","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1007/s12928-025-01136-3","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/5/27 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
摘要
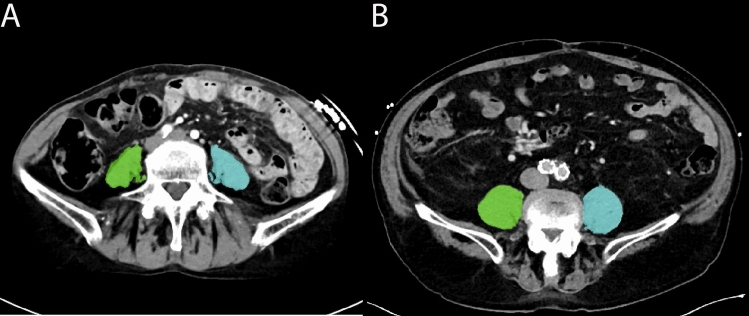
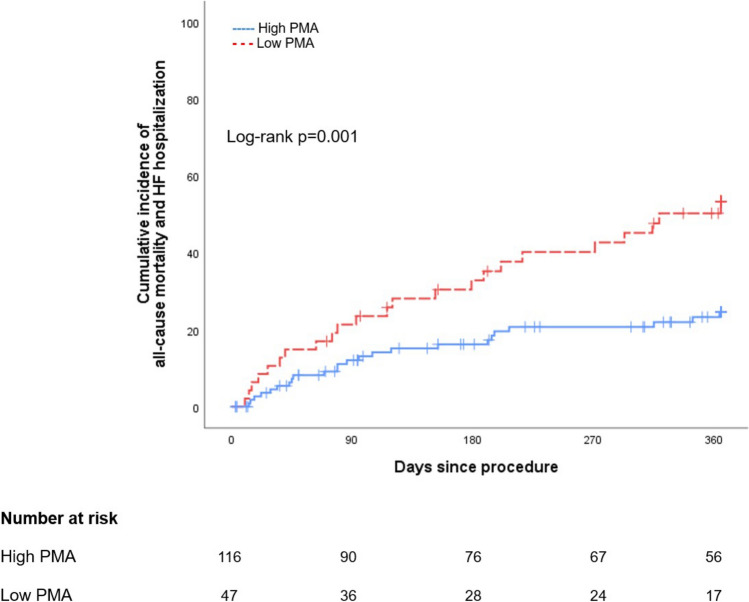
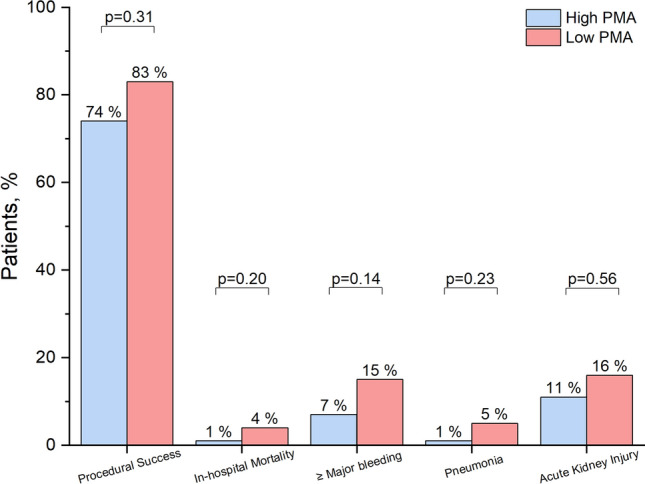
经导管三尖瓣修复(TTVR)可能是减少肌少症患者三尖瓣反流(TR)的另一种选择。腰肌面积(PMA)测量使用计算机断层扫描(CT)被称为肌肉减少症的标志。我们调查了PMA与TTVR后手术和临床结果的关系。我们回顾性地使用术前CT测量了TTVR患者的左、右PMA。低PMA被定义为男性总PMA 2和女性总PMA 2。主要终点是TTVR后一年内的全因死亡率和心力衰竭住院率。在163例患者中,47例(29%)被认为具有低PMA。手术成功率(出院时残余TR≤2 +)和住院死亡率在低PMA和高PMA患者之间具有可比性。低PMA患者的复合结局发生率高于高PMA患者(49% vs 21%;p = 0.001)在调整基线特征后,这种关联是一致的(调整风险比0.43;95%置信区间:0.23-0.80;p = 0.008)。相比之下,无论PMA如何,纽约心脏协会的功能分级从基线到三个月的随访都有所改善。大约30%接受TTVR的患者发现PMA较低。虽然TTVR可能是减少肌肉减少症患者TR和改善心力衰竭症状的一种安全的治疗选择,但在这一人群中,TTVR后的预后仍然很差。术前基于ct的PMA评估可以增强TTVR的风险分层,并支持更好的临床决策。
Association between psoas muscle area and outcomes after transcatheter tricuspid valve repair.
Transcatheter tricuspid valve repair (TTVR) might be an alternative option to reduce tricuspid regurgitation (TR) in patients with sarcopenia. Psoas muscle area (PMA) measured using computed tomography (CT) is known as a marker of sarcopenia. We investigated the association of PMA with procedural and clinical outcomes following TTVR. We retrospectively measured left and right PMA using pre-procedural CT in patients undergoing TTVR. Low PMA was defined as the total PMA < 20.3 cm2 for men and < 11.8 cm2 for women. The primary outcome was a composite of all-cause mortality and heart failure hospitalization within one year after TTVR. Of 163 patients, 47 (29%) were considered as having low PMA. Procedural success, defined as residual TR of ≤ 2 + at discharge, and in-hospital mortality were comparable between patients with low and high PMA. Patients with low PMA had a higher incidence of the composite outcome than those with high PMA (49% vs. 21%; p = 0.001) This association was consistent after adjusting for baseline characteristics (adjusted hazard ratio 0.43; 95% confidence interval: 0.23-0.80; p = 0.008). In contrast, the New York Heart Association functional class improved from baseline to three-month follow-up, regardless of PMA. Approximately 30% of patients undergoing TTVR were found to have low PMA. Although TTVR may be a safe therapeutic option to reduce TR and improve heart failure symptoms in patients with sarcopenia, the prognosis after TTVR remains poor in this population. Pre-procedural CT-based assessment of PMA may enhance risk stratification and support better clinical decision-making for TTVR.
期刊介绍:
Cardiovascular Intervention and Therapeutics (CVIT) is an international journal covering the field of cardiovascular disease and includes cardiac (coronary and noncoronary) and peripheral interventions and therapeutics. Articles are subject to peer review and complete editorial evaluation prior to any decision regarding acceptability. CVIT is an official journal of The Japanese Association of Cardiovascular Intervention and Therapeutics.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


