Ali Mansoursamaei, Maryam Valikhani, Hoofar Rafiee
{"title":"隐性内脏利什曼病患者的膜增生性肾小球肾炎的致命结局。","authors":"Ali Mansoursamaei, Maryam Valikhani, Hoofar Rafiee","doi":"10.1155/crdi/3448351","DOIUrl":null,"url":null,"abstract":"<p><p><b>Background:</b> Visceral leishmaniasis (VL) is a systemic parasitic disease with diverse clinical manifestations, primarily affecting the spleen, liver, and bone marrow. While renal involvement in VL is well documented, it is often mild and resolves with effective treatment. However, severe renal complications, such as membranoproliferative glomerulonephritis (MPGN), are rare and typically associated with immunocompromised individuals. <b>Case Report:</b> We report the case of a 30-year-old male from a nonendemic region who presented with unusual clinical features of generalized edema and abdominal pain, without the classic signs of VL such as fever or hepatosplenomegaly. Clinical examination, laboratory investigations, and other therapeutic interventions ruled out hepatic and cardiac causes of edema, focusing the diagnosis on nephrotic syndrome and acute kidney injury (AKI). A renal biopsy revealed MPGN, a rare but documented complication of VL. The presence of an autoimmune disease was suspected initially, and the patient was treated with steroids without improvement. The diagnosis of VL was confirmed only after bone marrow biopsy, which identified Leishmania amastigotes. Despite prompt initiation of antileishmanial therapy with liposomal amphotericin B, the patient's renal function continued to diminish, which finally resulted in end-stage renal disease (ESRD). The patient later developed pleural and pericardial effusion, pulmonary embolism, and tamponade, ultimately leading to a fatal outcome. <b>Conclusion:</b> This case underscores the importance of considering VL in the differential diagnosis of unexplained renal dysfunction, even in the absence of classic symptoms and in nonendemic regions. It highlights the potential for VL to present with atypical renal manifestations such as MPGN, leading to severe and irreversible renal damage if diagnosis and treatment are delayed. Early recognition and intervention are critical to improving outcomes in VL-associated renal disease.</p>","PeriodicalId":9608,"journal":{"name":"Case Reports in Infectious Diseases","volume":"2025 ","pages":"3448351"},"PeriodicalIF":0.8000,"publicationDate":"2025-05-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12105904/pdf/","citationCount":"0","resultStr":"{\"title\":\"Fatal Outcome of Membranoproliferative Glomerulonephritis in a Patient With Hidden Visceral Leishmaniasis.\",\"authors\":\"Ali Mansoursamaei, Maryam Valikhani, Hoofar Rafiee\",\"doi\":\"10.1155/crdi/3448351\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p><b>Background:</b> Visceral leishmaniasis (VL) is a systemic parasitic disease with diverse clinical manifestations, primarily affecting the spleen, liver, and bone marrow. While renal involvement in VL is well documented, it is often mild and resolves with effective treatment. However, severe renal complications, such as membranoproliferative glomerulonephritis (MPGN), are rare and typically associated with immunocompromised individuals. <b>Case Report:</b> We report the case of a 30-year-old male from a nonendemic region who presented with unusual clinical features of generalized edema and abdominal pain, without the classic signs of VL such as fever or hepatosplenomegaly. Clinical examination, laboratory investigations, and other therapeutic interventions ruled out hepatic and cardiac causes of edema, focusing the diagnosis on nephrotic syndrome and acute kidney injury (AKI). A renal biopsy revealed MPGN, a rare but documented complication of VL. The presence of an autoimmune disease was suspected initially, and the patient was treated with steroids without improvement. The diagnosis of VL was confirmed only after bone marrow biopsy, which identified Leishmania amastigotes. Despite prompt initiation of antileishmanial therapy with liposomal amphotericin B, the patient's renal function continued to diminish, which finally resulted in end-stage renal disease (ESRD). The patient later developed pleural and pericardial effusion, pulmonary embolism, and tamponade, ultimately leading to a fatal outcome. <b>Conclusion:</b> This case underscores the importance of considering VL in the differential diagnosis of unexplained renal dysfunction, even in the absence of classic symptoms and in nonendemic regions. It highlights the potential for VL to present with atypical renal manifestations such as MPGN, leading to severe and irreversible renal damage if diagnosis and treatment are delayed. Early recognition and intervention are critical to improving outcomes in VL-associated renal disease.</p>\",\"PeriodicalId\":9608,\"journal\":{\"name\":\"Case Reports in Infectious Diseases\",\"volume\":\"2025 \",\"pages\":\"3448351\"},\"PeriodicalIF\":0.8000,\"publicationDate\":\"2025-05-19\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12105904/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Case Reports in Infectious Diseases\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1155/crdi/3448351\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q4\",\"JCRName\":\"INFECTIOUS DISEASES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Infectious Diseases","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/crdi/3448351","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"INFECTIOUS DISEASES","Score":null,"Total":0}
Fatal Outcome of Membranoproliferative Glomerulonephritis in a Patient With Hidden Visceral Leishmaniasis.
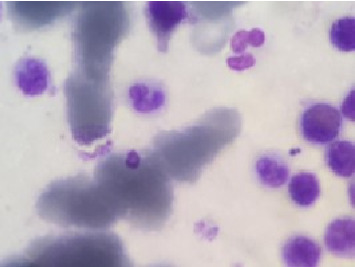
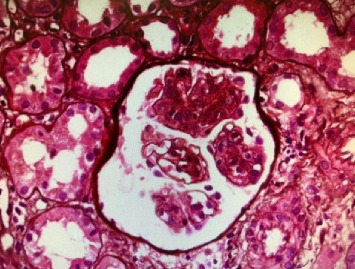
Background: Visceral leishmaniasis (VL) is a systemic parasitic disease with diverse clinical manifestations, primarily affecting the spleen, liver, and bone marrow. While renal involvement in VL is well documented, it is often mild and resolves with effective treatment. However, severe renal complications, such as membranoproliferative glomerulonephritis (MPGN), are rare and typically associated with immunocompromised individuals. Case Report: We report the case of a 30-year-old male from a nonendemic region who presented with unusual clinical features of generalized edema and abdominal pain, without the classic signs of VL such as fever or hepatosplenomegaly. Clinical examination, laboratory investigations, and other therapeutic interventions ruled out hepatic and cardiac causes of edema, focusing the diagnosis on nephrotic syndrome and acute kidney injury (AKI). A renal biopsy revealed MPGN, a rare but documented complication of VL. The presence of an autoimmune disease was suspected initially, and the patient was treated with steroids without improvement. The diagnosis of VL was confirmed only after bone marrow biopsy, which identified Leishmania amastigotes. Despite prompt initiation of antileishmanial therapy with liposomal amphotericin B, the patient's renal function continued to diminish, which finally resulted in end-stage renal disease (ESRD). The patient later developed pleural and pericardial effusion, pulmonary embolism, and tamponade, ultimately leading to a fatal outcome. Conclusion: This case underscores the importance of considering VL in the differential diagnosis of unexplained renal dysfunction, even in the absence of classic symptoms and in nonendemic regions. It highlights the potential for VL to present with atypical renal manifestations such as MPGN, leading to severe and irreversible renal damage if diagnosis and treatment are delayed. Early recognition and intervention are critical to improving outcomes in VL-associated renal disease.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


