东亚移民和房颤直接口服抗凝剂剂量:一项基于人群的队列研究。
IF 5.7
2区 医学
Q1 CARDIAC & CARDIOVASCULAR SYSTEMS
引用次数: 0
摘要
背景:一些东亚(EA)指南推荐的房颤(AF)直接口服抗凝剂(DOACs)的剂量低于北美和欧洲。目的:探讨EA移民与房房炎DOAC剂量和预后的关系。方法:使用安大略省行政数据库进行基于人群的队列研究,这些移民年龄≥66岁,在2012-2019年期间使用DOAC处方。出生国是否被归类为EA。我们使用多变量logistic回归来评估EA出生与DOAC剂量的关系,并使用病因特异性危险回归来评估EA出生和DOAC剂量与中风/出血/死亡的关系。研究了EA出生和DOAC剂量之间的相互作用。结果:在14,421名移民中,3958名(27.4%)出生在EA。EA移民接受全剂量DOACs的几率低于非EA移民(OR 0.64, 95%CI 0.58-0.69, p)结论:EA移民接受全剂量DOACs的可能性较低,出血风险较高,卒中风险相似,死亡风险低于非EA移民。没有证据表明DOAC剂量对EA移民有不同的治疗效果。本文章由计算机程序翻译,如有差异,请以英文原文为准。
East Asian immigration and direct oral anticoagulant dosing for atrial fibrillation: A population-based cohort study
Background
Some East Asian (EA) guidelines recommend lower doses of direct oral anticoagulants (DOACs) for atrial fibrillation (AF) than in North America and Europe.
Objective
The study aimed to investigate the association of immigration from EA with DOAC dosing and outcomes in AF.
Methods
This was a population-based cohort study using administrative databases of Ontario immigrants with AF aged ≥ 66 years who were dispensed DOAC prescriptions from 2012 to 2019. Birth country was classified as EA or not. We used multivariable logistic regression to assess the association of EA birth with DOAC dose and cause-specific hazards regression for the association of EA birth and DOAC dose with stroke or bleeding or death. The interaction between EA birth and DOAC dosing was studied for each outcome.
Results
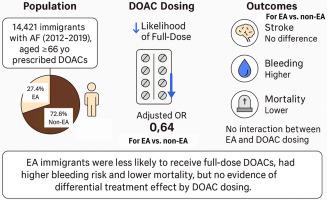
Among 14,421 immigrants, 3958 (27.4%) were born in EA. EA immigrants had lower odds of receiving full-dose DOACs vs non-EA immigrants (odds ratio 0.64, 95% confidence interval [CI] 0.58–0.69, P < .001). EA birth was not associated with a composite of hospitalization for stroke or bleeding (hazard ratio [HR] 0.97, 95% CI 0.84–1.12, P = .67) or hospitalization for stroke (HR 0.86, 95% CI 0.71–1.04, P = .13), but was associated with higher bleeding hazard (HR 1.15, 95% CI 1.02–1.30, P = .02) and lower mortality (HR 0.91, 95% CI 0.84–0.99, P = .04). There was no significant interaction between EA birth and DOAC dosing for stroke (P = .41), bleeding (P = .27), or death (P = .33).
Conclusions
EA immigrants were less likely to receive full-dose DOACs and had a higher bleeding hazard, similar stroke hazard, and lower mortality risk than non-EA immigrants. There was no evidence that DOAC dosing had a differential treatment effect in EA immigrants.
求助全文
通过发布文献求助,成功后即可免费获取论文全文。
去求助
来源期刊

Heart rhythm
医学-心血管系统
CiteScore
10.50
自引率
5.50%
发文量
1465
审稿时长
24 days
期刊介绍:
HeartRhythm, the official Journal of the Heart Rhythm Society and the Cardiac Electrophysiology Society, is a unique journal for fundamental discovery and clinical applicability.
HeartRhythm integrates the entire cardiac electrophysiology (EP) community from basic and clinical academic researchers, private practitioners, engineers, allied professionals, industry, and trainees, all of whom are vital and interdependent members of our EP community.
The Heart Rhythm Society is the international leader in science, education, and advocacy for cardiac arrhythmia professionals and patients, and the primary information resource on heart rhythm disorders. Its mission is to improve the care of patients by promoting research, education, and optimal health care policies and standards.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


