Vicka Poudyal, Marianne S Elston, Saleen Nottingham, Michael J Swarbrick, Adam Davies, Veronica Boyle
{"title":"肾神经内分泌肿瘤所致库欣综合征1例报告。","authors":"Vicka Poudyal, Marianne S Elston, Saleen Nottingham, Michael J Swarbrick, Adam Davies, Veronica Boyle","doi":"10.1159/000545734","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Cushing's syndrome (CS) due to ectopic adrenocorticotrophic hormone (ACTH) is rare and usually due to neuroendocrine neoplasia (NEN). Primary renal NEN is exceptionally rare but may be a cause of rapidly progressive CS.</p><p><strong>Case presentation: </strong>A 51-year-old man presented with profound hypokalemia, cellulitis, and new-onset type 2 diabetes and hypertension with 1 month of muscle weakness, labile mood, and insomnia. CS due to ectopic ACTH production was confirmed. Biochemical control was achieved using a \"block-and-replace\" regimen with dual blockade with ketoconazole and metyrapone and hydrocortisone replacement in addition to mineralocorticoid receptor blockade using spironolactone. CT and ultrasound demonstrated a 24 mm right renal lesion with features concerning for renal cell carcinoma. Right laparoscopic nephrectomy was performed. Histology demonstrated a WHO grade one NEN with ACTH staining.</p><p><strong>Conclusion: </strong>In CS, where the source of ectopic ACTH production is unable to be identified, a renal source should be considered. Diagnosis may be difficult as there are no reliable radiological characteristics to distinguish renal NENs from renal cell carcinomas, so a high degree of suspicion is required.</p>","PeriodicalId":9625,"journal":{"name":"Case Reports in Oncology","volume":"18 1","pages":"593-601"},"PeriodicalIF":0.7000,"publicationDate":"2025-04-14","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12101822/pdf/","citationCount":"0","resultStr":"{\"title\":\"Cushing's Syndrome due to a Renal Neuroendocrine Tumor: A Case Report.\",\"authors\":\"Vicka Poudyal, Marianne S Elston, Saleen Nottingham, Michael J Swarbrick, Adam Davies, Veronica Boyle\",\"doi\":\"10.1159/000545734\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Cushing's syndrome (CS) due to ectopic adrenocorticotrophic hormone (ACTH) is rare and usually due to neuroendocrine neoplasia (NEN). Primary renal NEN is exceptionally rare but may be a cause of rapidly progressive CS.</p><p><strong>Case presentation: </strong>A 51-year-old man presented with profound hypokalemia, cellulitis, and new-onset type 2 diabetes and hypertension with 1 month of muscle weakness, labile mood, and insomnia. CS due to ectopic ACTH production was confirmed. Biochemical control was achieved using a \\\"block-and-replace\\\" regimen with dual blockade with ketoconazole and metyrapone and hydrocortisone replacement in addition to mineralocorticoid receptor blockade using spironolactone. CT and ultrasound demonstrated a 24 mm right renal lesion with features concerning for renal cell carcinoma. Right laparoscopic nephrectomy was performed. Histology demonstrated a WHO grade one NEN with ACTH staining.</p><p><strong>Conclusion: </strong>In CS, where the source of ectopic ACTH production is unable to be identified, a renal source should be considered. Diagnosis may be difficult as there are no reliable radiological characteristics to distinguish renal NENs from renal cell carcinomas, so a high degree of suspicion is required.</p>\",\"PeriodicalId\":9625,\"journal\":{\"name\":\"Case Reports in Oncology\",\"volume\":\"18 1\",\"pages\":\"593-601\"},\"PeriodicalIF\":0.7000,\"publicationDate\":\"2025-04-14\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12101822/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Case Reports in Oncology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1159/000545734\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q4\",\"JCRName\":\"ONCOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Oncology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1159/000545734","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"ONCOLOGY","Score":null,"Total":0}
Cushing's Syndrome due to a Renal Neuroendocrine Tumor: A Case Report.
Introduction: Cushing's syndrome (CS) due to ectopic adrenocorticotrophic hormone (ACTH) is rare and usually due to neuroendocrine neoplasia (NEN). Primary renal NEN is exceptionally rare but may be a cause of rapidly progressive CS.
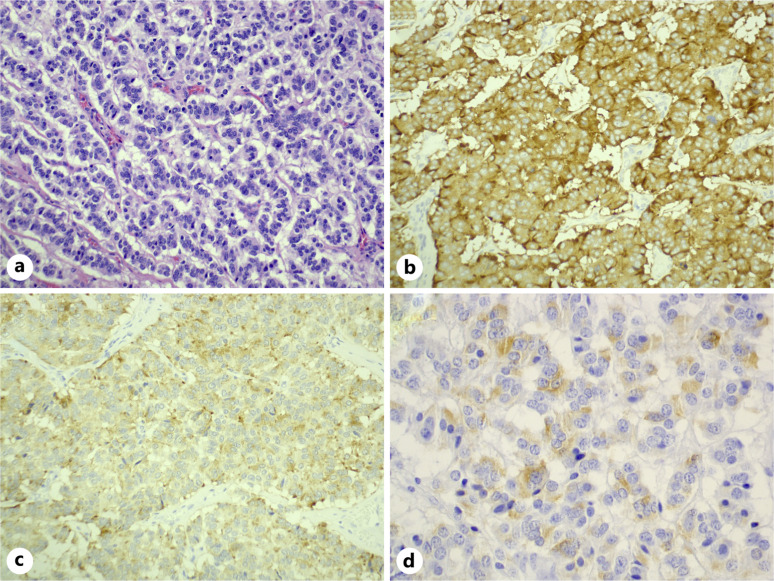
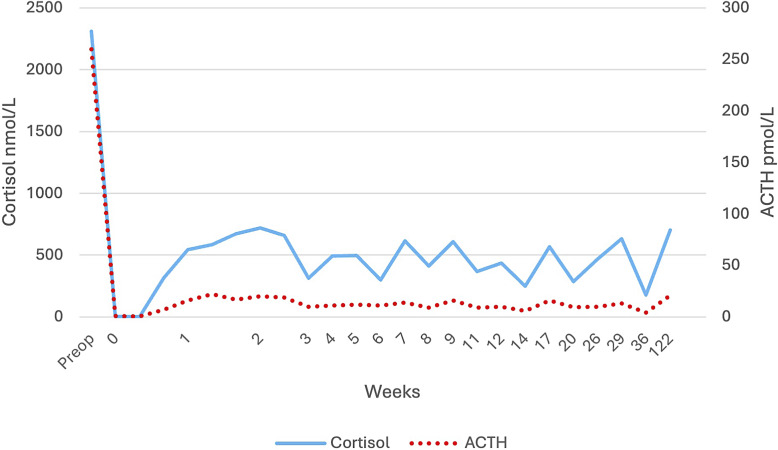
Case presentation: A 51-year-old man presented with profound hypokalemia, cellulitis, and new-onset type 2 diabetes and hypertension with 1 month of muscle weakness, labile mood, and insomnia. CS due to ectopic ACTH production was confirmed. Biochemical control was achieved using a "block-and-replace" regimen with dual blockade with ketoconazole and metyrapone and hydrocortisone replacement in addition to mineralocorticoid receptor blockade using spironolactone. CT and ultrasound demonstrated a 24 mm right renal lesion with features concerning for renal cell carcinoma. Right laparoscopic nephrectomy was performed. Histology demonstrated a WHO grade one NEN with ACTH staining.
Conclusion: In CS, where the source of ectopic ACTH production is unable to be identified, a renal source should be considered. Diagnosis may be difficult as there are no reliable radiological characteristics to distinguish renal NENs from renal cell carcinomas, so a high degree of suspicion is required.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


