Cristian-Vladimir Vancea, Florin-Vlad Hodea, Eliza-Maria Bordeanu-Diaconescu, Stefan Cacior, Catalina-Stefania Dumitru, Vladut-Alin Ratoiu, Alexandru Stoian, Ioan Lascar, Dragos Zamfirescu
{"title":"神经转移治疗臂丛损伤肩肘复位后的功能结局:一项10年回顾性研究。","authors":"Cristian-Vladimir Vancea, Florin-Vlad Hodea, Eliza-Maria Bordeanu-Diaconescu, Stefan Cacior, Catalina-Stefania Dumitru, Vladut-Alin Ratoiu, Alexandru Stoian, Ioan Lascar, Dragos Zamfirescu","doi":"10.25122/jml-2025-0079","DOIUrl":null,"url":null,"abstract":"<p><p>Brachial plexus injuries are rare but highly disabling, with major implications for upper limb function and quality of life. Nerve transfers have emerged as a key reconstructive technique, particularly valuable in cases where primary repair or grafting is unfeasible or delayed. This retrospective study analysed functional outcomes following nerve transfers in 37 patients with brachial plexus injury. Motor recovery was assessed using the Medical Research Council scale. Patients were stratified by age, timing of surgery, injury severity, and type of nerve transfer performed. The majority of our cohort consisted of male adults, predominantly injured in motorcycle accidents, while pediatric cases were mostly due to obstetrical trauma. For shoulder reanimation, all patients received spinal accessory to suprascapular nerve transfer, with a subset also undergoing medial triceps branch of the radial nerve to axillary nerve transfer. These techniques resulted in 85.3% of patients achieving shoulder function recovery with M3 or M4 muscle strength, with combined procedures leading exclusively to M3 or M4 muscle strength. For elbow flexion restoration, surgical approaches included intercostal to musculocutaneous nerve transfer, ulnar and median fascicles to musculocutaneous nerve transfer, contralateral C7 to musculocutaneous nerve transfer with ulnar graft, and spinal accessory to musculocutaneous nerve transfer with sural nerve graft. Root grafting procedures using sural nerve grafts or nerve conduits were employed in three pediatric patients. Overall, 84.38% of patients achieved elbow flexion recovery with M3 or M4 muscle strength. These findings reinforce the utility of nerve transfers as a cornerstone in the surgical management of brachial plexus injury.</p>","PeriodicalId":16386,"journal":{"name":"Journal of Medicine and Life","volume":"18 4","pages":"375-386"},"PeriodicalIF":0.0000,"publicationDate":"2025-04-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12094303/pdf/","citationCount":"0","resultStr":"{\"title\":\"Functional outcomes following nerve transfers for shoulder and elbow reanimation in brachial plexus injuries: a 10-year retrospective study.\",\"authors\":\"Cristian-Vladimir Vancea, Florin-Vlad Hodea, Eliza-Maria Bordeanu-Diaconescu, Stefan Cacior, Catalina-Stefania Dumitru, Vladut-Alin Ratoiu, Alexandru Stoian, Ioan Lascar, Dragos Zamfirescu\",\"doi\":\"10.25122/jml-2025-0079\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Brachial plexus injuries are rare but highly disabling, with major implications for upper limb function and quality of life. Nerve transfers have emerged as a key reconstructive technique, particularly valuable in cases where primary repair or grafting is unfeasible or delayed. This retrospective study analysed functional outcomes following nerve transfers in 37 patients with brachial plexus injury. Motor recovery was assessed using the Medical Research Council scale. Patients were stratified by age, timing of surgery, injury severity, and type of nerve transfer performed. The majority of our cohort consisted of male adults, predominantly injured in motorcycle accidents, while pediatric cases were mostly due to obstetrical trauma. For shoulder reanimation, all patients received spinal accessory to suprascapular nerve transfer, with a subset also undergoing medial triceps branch of the radial nerve to axillary nerve transfer. These techniques resulted in 85.3% of patients achieving shoulder function recovery with M3 or M4 muscle strength, with combined procedures leading exclusively to M3 or M4 muscle strength. For elbow flexion restoration, surgical approaches included intercostal to musculocutaneous nerve transfer, ulnar and median fascicles to musculocutaneous nerve transfer, contralateral C7 to musculocutaneous nerve transfer with ulnar graft, and spinal accessory to musculocutaneous nerve transfer with sural nerve graft. Root grafting procedures using sural nerve grafts or nerve conduits were employed in three pediatric patients. Overall, 84.38% of patients achieved elbow flexion recovery with M3 or M4 muscle strength. These findings reinforce the utility of nerve transfers as a cornerstone in the surgical management of brachial plexus injury.</p>\",\"PeriodicalId\":16386,\"journal\":{\"name\":\"Journal of Medicine and Life\",\"volume\":\"18 4\",\"pages\":\"375-386\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2025-04-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12094303/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Medicine and Life\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.25122/jml-2025-0079\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Medicine and Life","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.25122/jml-2025-0079","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"Medicine","Score":null,"Total":0}
Functional outcomes following nerve transfers for shoulder and elbow reanimation in brachial plexus injuries: a 10-year retrospective study.
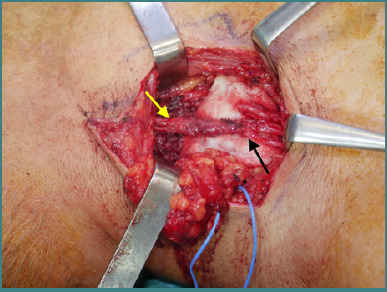
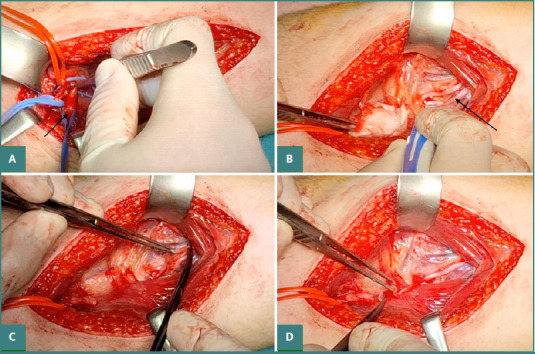
Brachial plexus injuries are rare but highly disabling, with major implications for upper limb function and quality of life. Nerve transfers have emerged as a key reconstructive technique, particularly valuable in cases where primary repair or grafting is unfeasible or delayed. This retrospective study analysed functional outcomes following nerve transfers in 37 patients with brachial plexus injury. Motor recovery was assessed using the Medical Research Council scale. Patients were stratified by age, timing of surgery, injury severity, and type of nerve transfer performed. The majority of our cohort consisted of male adults, predominantly injured in motorcycle accidents, while pediatric cases were mostly due to obstetrical trauma. For shoulder reanimation, all patients received spinal accessory to suprascapular nerve transfer, with a subset also undergoing medial triceps branch of the radial nerve to axillary nerve transfer. These techniques resulted in 85.3% of patients achieving shoulder function recovery with M3 or M4 muscle strength, with combined procedures leading exclusively to M3 or M4 muscle strength. For elbow flexion restoration, surgical approaches included intercostal to musculocutaneous nerve transfer, ulnar and median fascicles to musculocutaneous nerve transfer, contralateral C7 to musculocutaneous nerve transfer with ulnar graft, and spinal accessory to musculocutaneous nerve transfer with sural nerve graft. Root grafting procedures using sural nerve grafts or nerve conduits were employed in three pediatric patients. Overall, 84.38% of patients achieved elbow flexion recovery with M3 or M4 muscle strength. These findings reinforce the utility of nerve transfers as a cornerstone in the surgical management of brachial plexus injury.
期刊介绍:
The Journal of Medicine and Life publishes peer-reviewed articles from various fields of medicine and life sciences, including original research, systematic reviews, special reports, case presentations, major medical breakthroughs and letters to the editor. The Journal focuses on current matters that lie at the intersection of biomedical science and clinical practice and strives to present this information to inform health care delivery and improve patient outcomes. Papers addressing topics such as neuroprotection, neurorehabilitation, neuroplasticity, and neuroregeneration are particularly encouraged, as part of the Journal''s continuous interest in neuroscience research. The Editorial Board of the Journal of Medicine and Life is open to consider manuscripts from all levels of research and areas of biological sciences, including fundamental, experimental or clinical research and matters of public health. As part of our pledge to promote an educational and community-building environment, our issues feature sections designated to informing our readers regarding exciting international congresses, teaching courses and relevant institutional-level events.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


