Gaurav Suryawanshi, Megan B Ghai, Nauroze Faizi, Stuart K Amateau, Nabeel Azeem, Shawn Mallery, Martin L Freeman, Guru Trikudanathan
{"title":"坏死性胰腺炎30天意外再入院的预测因素——来自三级保健中心的12年经验。","authors":"Gaurav Suryawanshi, Megan B Ghai, Nauroze Faizi, Stuart K Amateau, Nabeel Azeem, Shawn Mallery, Martin L Freeman, Guru Trikudanathan","doi":"10.14309/ctg.0000000000000848","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Hospital readmission rate is a key hospital metric and represents a substantial burden to patients and the healthcare system. Necrotizing pancreatitis (NP) patients are at high risk of unplanned readmission. The aim of this study was to determine the incidence and predictors of 30-day unplanned readmission after index hospitalization for NP.</p><p><strong>Methods: </strong>Adult NP patients who were managed at a single tertiary referral center between 2009 and 2022 were identified from a prospective database and categorized into 2 groups based on 30-day unplanned readmission after index hospitalization. Patients with no follow-up who died during index admission or within 30 days of discharge were excluded. Baseline data on admission including demographic, clinical, interventional, imaging, and discharge characteristics were compared. Multivariable analysis was completed to identify independent predictors of 30-day readmission.</p><p><strong>Results: </strong>Among 505 patients with NP (male patients-347 [69%], median age-50 years [inter quartile range 37-63]) 191 (37.8%) had at least 1 unplanned readmission. The most common causes of readmission were abdominal pain (40%) and sepsis (27%). On multivariable analysis, independent predictors for early readmission were necrosis collection size ≥ 6 cm (adjusted odds ratio [aOR] 1.91 [1.11-3.30], P < 0.03), stay at outside hospital ≥ 14 days before transfer to tertiary center (aOR 2.89 [1.27-6.60], P < 0.01), and need for percutaneous feeding tube at the time of discharge (aOR 2.06 [1.01-4.21], P < 0.05).</p><p><strong>Discussion: </strong>Readmission after NP is common and associated with greater mortality at 6 months. Expedited transfer to tertiary center for timely intervention, assiduous follow-up of other high-risk patients (large collections and those who need enteral nutrition) could help avoid readmissions and optimize outcomes.</p>","PeriodicalId":10278,"journal":{"name":"Clinical and Translational Gastroenterology","volume":" ","pages":"e00848"},"PeriodicalIF":3.0000,"publicationDate":"2025-05-23","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12330361/pdf/","citationCount":"0","resultStr":"{\"title\":\"Predictors of 30-Day Unplanned Readmission in Necrotizing Pancreatitis: A 12-Year Experience From a Tertiary Care Center.\",\"authors\":\"Gaurav Suryawanshi, Megan B Ghai, Nauroze Faizi, Stuart K Amateau, Nabeel Azeem, Shawn Mallery, Martin L Freeman, Guru Trikudanathan\",\"doi\":\"10.14309/ctg.0000000000000848\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Hospital readmission rate is a key hospital metric and represents a substantial burden to patients and the healthcare system. Necrotizing pancreatitis (NP) patients are at high risk of unplanned readmission. The aim of this study was to determine the incidence and predictors of 30-day unplanned readmission after index hospitalization for NP.</p><p><strong>Methods: </strong>Adult NP patients who were managed at a single tertiary referral center between 2009 and 2022 were identified from a prospective database and categorized into 2 groups based on 30-day unplanned readmission after index hospitalization. Patients with no follow-up who died during index admission or within 30 days of discharge were excluded. Baseline data on admission including demographic, clinical, interventional, imaging, and discharge characteristics were compared. Multivariable analysis was completed to identify independent predictors of 30-day readmission.</p><p><strong>Results: </strong>Among 505 patients with NP (male patients-347 [69%], median age-50 years [inter quartile range 37-63]) 191 (37.8%) had at least 1 unplanned readmission. The most common causes of readmission were abdominal pain (40%) and sepsis (27%). On multivariable analysis, independent predictors for early readmission were necrosis collection size ≥ 6 cm (adjusted odds ratio [aOR] 1.91 [1.11-3.30], P < 0.03), stay at outside hospital ≥ 14 days before transfer to tertiary center (aOR 2.89 [1.27-6.60], P < 0.01), and need for percutaneous feeding tube at the time of discharge (aOR 2.06 [1.01-4.21], P < 0.05).</p><p><strong>Discussion: </strong>Readmission after NP is common and associated with greater mortality at 6 months. Expedited transfer to tertiary center for timely intervention, assiduous follow-up of other high-risk patients (large collections and those who need enteral nutrition) could help avoid readmissions and optimize outcomes.</p>\",\"PeriodicalId\":10278,\"journal\":{\"name\":\"Clinical and Translational Gastroenterology\",\"volume\":\" \",\"pages\":\"e00848\"},\"PeriodicalIF\":3.0000,\"publicationDate\":\"2025-05-23\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12330361/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical and Translational Gastroenterology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.14309/ctg.0000000000000848\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/7/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical and Translational Gastroenterology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.14309/ctg.0000000000000848","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/7/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
背景和目的:医院再入院率是医院的一项关键指标,对患者和卫生保健系统来说是一个巨大的负担。坏死性胰腺炎(NP)患者意外再入院的风险很高。本研究的目的是确定NP指数住院后30天意外再入院的发生率和预测因素。方法:从前瞻性数据库中确定2009-2022年间在单一三级转诊中心治疗的成年NP患者,并根据指数住院后30天的计划外再入院分为两组。排除无随访、入院时死亡或出院30天内死亡的患者。入院的基线数据包括人口学、临床、介入、影像学和出院特征进行比较。完成多变量分析以确定30天再入院的独立预测因素。结果:505例NP患者中,[男性347例(69%),中位年龄- 50岁(IQR 37-63)] 191例(37.8%)至少有一次计划外再入院。再入院最常见的原因是腹痛(40%)和败血症(27%)。在多变量分析中,早期再入院的独立预测因子是坏死集合大小≥6 cm [aOR 1.91 (1.11-3.30), p]。结论:NP后再入院很常见,且与6个月时更高的死亡率相关。加快转移到三级中心及时干预,对其他高危患者(大量收集和需要肠内营养的患者)进行积极随访,有助于避免再入院和优化结果。
Predictors of 30-Day Unplanned Readmission in Necrotizing Pancreatitis: A 12-Year Experience From a Tertiary Care Center.
Introduction: Hospital readmission rate is a key hospital metric and represents a substantial burden to patients and the healthcare system. Necrotizing pancreatitis (NP) patients are at high risk of unplanned readmission. The aim of this study was to determine the incidence and predictors of 30-day unplanned readmission after index hospitalization for NP.
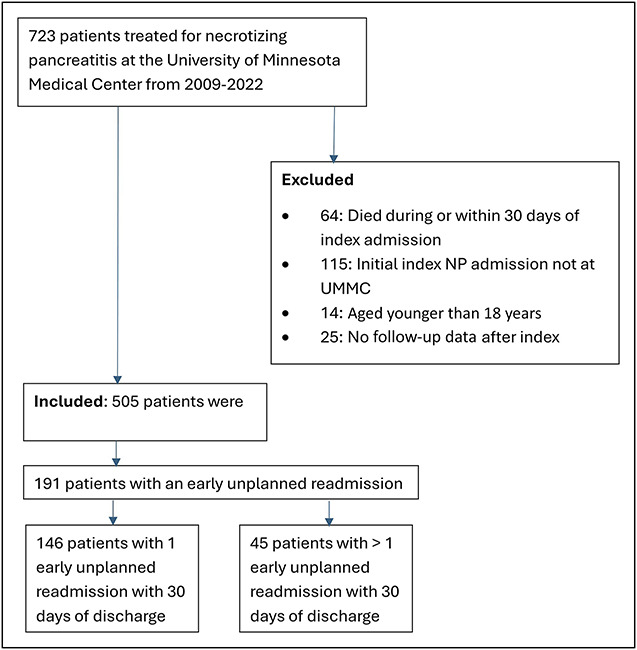
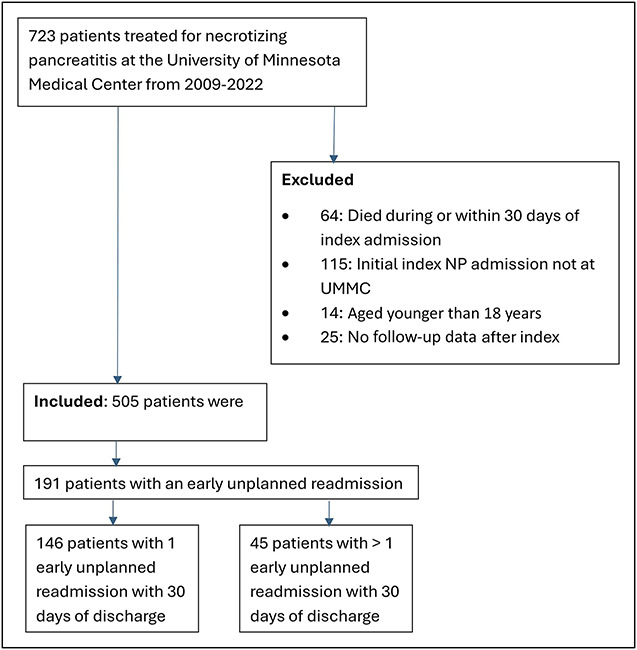
Methods: Adult NP patients who were managed at a single tertiary referral center between 2009 and 2022 were identified from a prospective database and categorized into 2 groups based on 30-day unplanned readmission after index hospitalization. Patients with no follow-up who died during index admission or within 30 days of discharge were excluded. Baseline data on admission including demographic, clinical, interventional, imaging, and discharge characteristics were compared. Multivariable analysis was completed to identify independent predictors of 30-day readmission.
Results: Among 505 patients with NP (male patients-347 [69%], median age-50 years [inter quartile range 37-63]) 191 (37.8%) had at least 1 unplanned readmission. The most common causes of readmission were abdominal pain (40%) and sepsis (27%). On multivariable analysis, independent predictors for early readmission were necrosis collection size ≥ 6 cm (adjusted odds ratio [aOR] 1.91 [1.11-3.30], P < 0.03), stay at outside hospital ≥ 14 days before transfer to tertiary center (aOR 2.89 [1.27-6.60], P < 0.01), and need for percutaneous feeding tube at the time of discharge (aOR 2.06 [1.01-4.21], P < 0.05).
Discussion: Readmission after NP is common and associated with greater mortality at 6 months. Expedited transfer to tertiary center for timely intervention, assiduous follow-up of other high-risk patients (large collections and those who need enteral nutrition) could help avoid readmissions and optimize outcomes.
期刊介绍:
Clinical and Translational Gastroenterology (CTG), published on behalf of the American College of Gastroenterology (ACG), is a peer-reviewed open access online journal dedicated to innovative clinical work in the field of gastroenterology and hepatology. CTG hopes to fulfill an unmet need for clinicians and scientists by welcoming novel cohort studies, early-phase clinical trials, qualitative and quantitative epidemiologic research, hypothesis-generating research, studies of novel mechanisms and methodologies including public health interventions, and integration of approaches across organs and disciplines. CTG also welcomes hypothesis-generating small studies, methods papers, and translational research with clear applications to human physiology or disease.
Colon and small bowel
Endoscopy and novel diagnostics
Esophagus
Functional GI disorders
Immunology of the GI tract
Microbiology of the GI tract
Inflammatory bowel disease
Pancreas and biliary tract
Liver
Pathology
Pediatrics
Preventative medicine
Nutrition/obesity
Stomach.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


