Pardis Seyedi, Dionne Aleman, Nancy N Baxter, Chaim M Bell, Merve Bodur, Andrew Calzavara, Robert Campbell, Michael Carter, Pieter de Jager, Scott D Emerson, Jonathan Irish, Danielle Martin, Samantha Lee, Jonathan Persitz, Marcy Saxe-Braithwaite, Julie Takata, Olivia Varkul, Suting Yang, Claudia Zanchetta, David R Urbach
{"title":"安大略省单次转诊模式和团队护理对髋关节和膝关节置换术等待时间的影响:一项模拟研究。","authors":"Pardis Seyedi, Dionne Aleman, Nancy N Baxter, Chaim M Bell, Merve Bodur, Andrew Calzavara, Robert Campbell, Michael Carter, Pieter de Jager, Scott D Emerson, Jonathan Irish, Danielle Martin, Samantha Lee, Jonathan Persitz, Marcy Saxe-Braithwaite, Julie Takata, Olivia Varkul, Suting Yang, Claudia Zanchetta, David R Urbach","doi":"10.1503/cmaj.241755","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Long wait times for scheduled surgery are a major problem in Canadian health systems. We sought to determine the extent to which single-entry referral models (next available consultation), team-based care models (next available surgery regardless of consulting surgeon), or both could affect wait times for consultations and surgery.</p><p><strong>Methods: </strong>We performed a discrete-event simulation study of wait times for consultations and surgeries for knee and hip joint replacement in Ontario's 5 postal regions using prospectively collected data on surgical wait times. We simulated the effects of coordinated referral models on the wait time for consultation (wait 1) and surgery (wait 2).</p><p><strong>Results: </strong>Coordinated models led to larger reductions in high-outlier wait times (as reflected by the 90th percentile and the percentage of patients exceeding wait-time targets) than on median wait times when compared with the status quo. Single-entry referral models largely influenced wait 1, and team-based models of care affected only wait 2. Fully integrated models incorporating both single-entry referral and team-based care largely prevented patients from exceeding both wait-1 and wait-2 targets; the percentage of patients exceeding wait-1 targets in these models was 0% in all regions, and the percentage exceeding wait-2 targets was 0% except for Ontario West (2.0%, from 35.7% at baseline), East (1.1%, from 22.7% at baseline), and North (1.0%, from 25.1% at baseline).</p><p><strong>Interpretation: </strong>Coordinated referral and practice models improve access to scheduled surgery in Canadian health systems. Implementation of these models could largely eliminate prolonged wait times for joint replacement surgery in Ontario.</p>","PeriodicalId":9609,"journal":{"name":"Canadian Medical Association journal","volume":"197 19","pages":"E524-E531"},"PeriodicalIF":11.3000,"publicationDate":"2025-05-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12109095/pdf/","citationCount":"0","resultStr":"{\"title\":\"Effect of single-entry referral models and team-based care on wait times for hip and knee joint replacement in Ontario: a simulation study.\",\"authors\":\"Pardis Seyedi, Dionne Aleman, Nancy N Baxter, Chaim M Bell, Merve Bodur, Andrew Calzavara, Robert Campbell, Michael Carter, Pieter de Jager, Scott D Emerson, Jonathan Irish, Danielle Martin, Samantha Lee, Jonathan Persitz, Marcy Saxe-Braithwaite, Julie Takata, Olivia Varkul, Suting Yang, Claudia Zanchetta, David R Urbach\",\"doi\":\"10.1503/cmaj.241755\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Long wait times for scheduled surgery are a major problem in Canadian health systems. We sought to determine the extent to which single-entry referral models (next available consultation), team-based care models (next available surgery regardless of consulting surgeon), or both could affect wait times for consultations and surgery.</p><p><strong>Methods: </strong>We performed a discrete-event simulation study of wait times for consultations and surgeries for knee and hip joint replacement in Ontario's 5 postal regions using prospectively collected data on surgical wait times. We simulated the effects of coordinated referral models on the wait time for consultation (wait 1) and surgery (wait 2).</p><p><strong>Results: </strong>Coordinated models led to larger reductions in high-outlier wait times (as reflected by the 90th percentile and the percentage of patients exceeding wait-time targets) than on median wait times when compared with the status quo. Single-entry referral models largely influenced wait 1, and team-based models of care affected only wait 2. Fully integrated models incorporating both single-entry referral and team-based care largely prevented patients from exceeding both wait-1 and wait-2 targets; the percentage of patients exceeding wait-1 targets in these models was 0% in all regions, and the percentage exceeding wait-2 targets was 0% except for Ontario West (2.0%, from 35.7% at baseline), East (1.1%, from 22.7% at baseline), and North (1.0%, from 25.1% at baseline).</p><p><strong>Interpretation: </strong>Coordinated referral and practice models improve access to scheduled surgery in Canadian health systems. Implementation of these models could largely eliminate prolonged wait times for joint replacement surgery in Ontario.</p>\",\"PeriodicalId\":9609,\"journal\":{\"name\":\"Canadian Medical Association journal\",\"volume\":\"197 19\",\"pages\":\"E524-E531\"},\"PeriodicalIF\":11.3000,\"publicationDate\":\"2025-05-19\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12109095/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Canadian Medical Association journal\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1503/cmaj.241755\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"MEDICINE, GENERAL & INTERNAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Canadian Medical Association journal","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1503/cmaj.241755","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
Effect of single-entry referral models and team-based care on wait times for hip and knee joint replacement in Ontario: a simulation study.
Background: Long wait times for scheduled surgery are a major problem in Canadian health systems. We sought to determine the extent to which single-entry referral models (next available consultation), team-based care models (next available surgery regardless of consulting surgeon), or both could affect wait times for consultations and surgery.
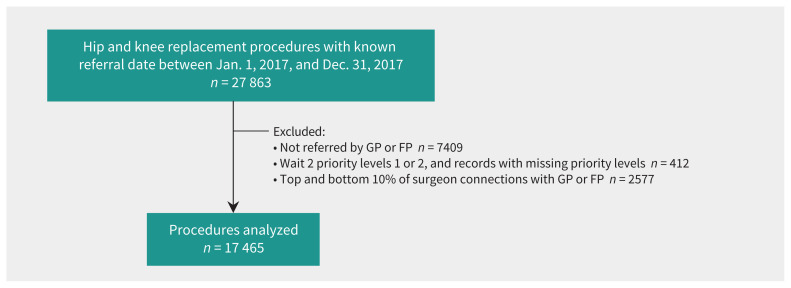
Methods: We performed a discrete-event simulation study of wait times for consultations and surgeries for knee and hip joint replacement in Ontario's 5 postal regions using prospectively collected data on surgical wait times. We simulated the effects of coordinated referral models on the wait time for consultation (wait 1) and surgery (wait 2).
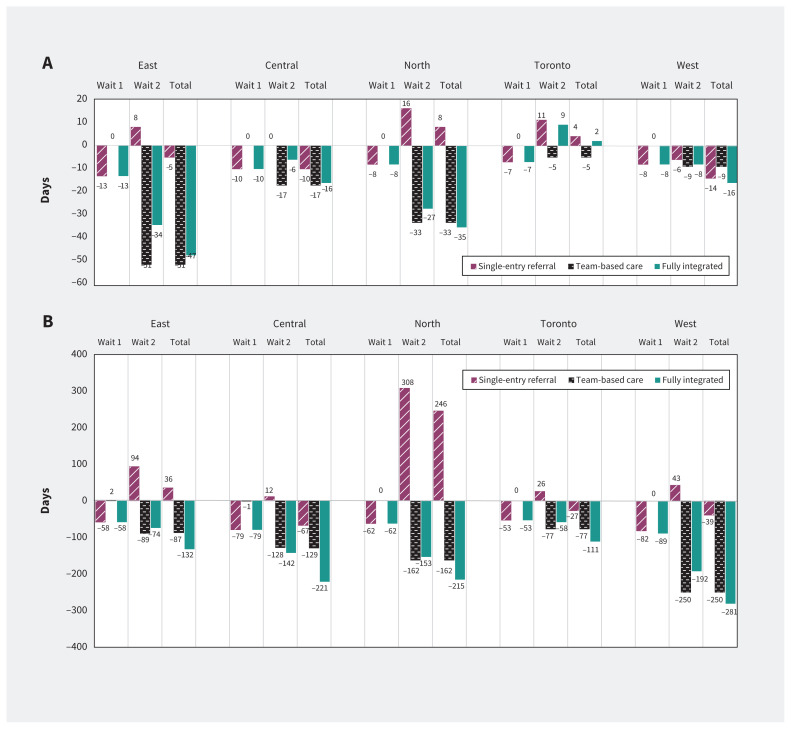
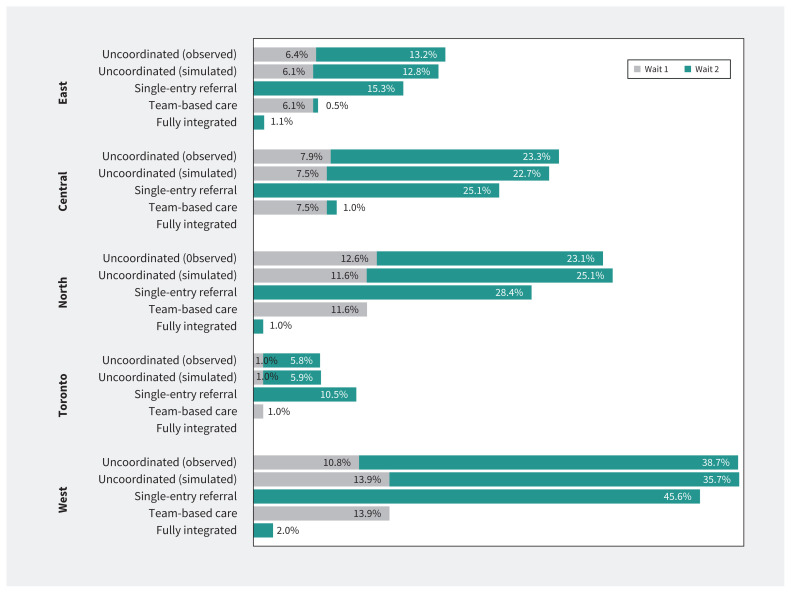
Results: Coordinated models led to larger reductions in high-outlier wait times (as reflected by the 90th percentile and the percentage of patients exceeding wait-time targets) than on median wait times when compared with the status quo. Single-entry referral models largely influenced wait 1, and team-based models of care affected only wait 2. Fully integrated models incorporating both single-entry referral and team-based care largely prevented patients from exceeding both wait-1 and wait-2 targets; the percentage of patients exceeding wait-1 targets in these models was 0% in all regions, and the percentage exceeding wait-2 targets was 0% except for Ontario West (2.0%, from 35.7% at baseline), East (1.1%, from 22.7% at baseline), and North (1.0%, from 25.1% at baseline).
Interpretation: Coordinated referral and practice models improve access to scheduled surgery in Canadian health systems. Implementation of these models could largely eliminate prolonged wait times for joint replacement surgery in Ontario.
期刊介绍:
CMAJ (Canadian Medical Association Journal) is a peer-reviewed general medical journal renowned for publishing original research, commentaries, analyses, reviews, clinical practice updates, and editorials. Led by Editor-in-Chief Dr. Kirsten Patrick, it has a significant impact on healthcare in Canada and globally, with a 2022 impact factor of 17.4.
Its mission is to promote knowledge vital for the health of Canadians and the global community, guided by values of service, evidence, and integrity. The journal's vision emphasizes the importance of the best evidence, practice, and health outcomes.
CMAJ covers a broad range of topics, focusing on contributing to the evidence base, influencing clinical practice, and raising awareness of pressing health issues among policymakers and the public. Since 2020, with the appointment of a Lead of Patient Involvement, CMAJ is committed to integrating patients into its governance and operations, encouraging their content submissions.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


