Radhika Duggal, Sarah Benyo, Elizabeth N Dewey, Rebecca C Nelson, Paul C Bryson, Michael S Benninger, Brandon Hopkins, William S Tierney
{"title":"气管切开术后住院处置的差异:一项全国分析。","authors":"Radhika Duggal, Sarah Benyo, Elizabeth N Dewey, Rebecca C Nelson, Paul C Bryson, Michael S Benninger, Brandon Hopkins, William S Tierney","doi":"10.1002/oto2.70129","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>Previous studies have demonstrated the impact of sociodemographic factors on disease development, management, and outcomes in adult and pediatric populations. Given that postoperative management is key in reducing complications following a tracheotomy, we assessed the impact of sociodemographic factors on a patient's discharge disposition.</p><p><strong>Study design: </strong>Cross-sectional study.</p><p><strong>Setting: </strong>Health Care Utilization Project's (HCUP) National Inpatient Survey (NIS).</p><p><strong>Methods: </strong>The HCUP NIS was queried for all patients undergoing tracheotomy between 2017 and 2021. All analyses were performed using R Version 4.3.1 survey procedures to account for strata and cluster effects.</p><p><strong>Results: </strong>We identified 81,069 admissions during which a tracheotomy was performed and, after appropriate weighting for the HCUP NIS survey design, found that 15.1% of admissions resulted in routine discharge, 4.5% transferred to a short-term hospital, 52.3% transferred to a skilled nursing facility (SNF)/intermediate care facility (ICF)/other facility, 16.9% discharged with home health care. Admissions routinely discharged had the lowest median (interquartile range) age (48 [23, 61] years), whereas admissions resulting in death or transfer to a SNF/ICF/other facility type had the greatest age (63 [53, 70] years). On both univariable and multivariable analyses, age, race, sex, insurance type, geographic region, and hospital size were associated with discharge disposition.</p><p><strong>Conclusion: </strong>Our study highlights that disparities exist among patient populations and were found in both unadjusted and adjusted analyses. Further attention and resource allocation for the care of patients with a tracheostomy may work toward identifying sources of disparity, which may be modified to improve patient care.</p>","PeriodicalId":19697,"journal":{"name":"OTO Open","volume":"9 2","pages":"e70129"},"PeriodicalIF":1.8000,"publicationDate":"2025-05-16","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12082083/pdf/","citationCount":"0","resultStr":"{\"title\":\"Disparities in Posthospitalization Disposition Following Tracheotomy: A National Analysis.\",\"authors\":\"Radhika Duggal, Sarah Benyo, Elizabeth N Dewey, Rebecca C Nelson, Paul C Bryson, Michael S Benninger, Brandon Hopkins, William S Tierney\",\"doi\":\"10.1002/oto2.70129\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>Previous studies have demonstrated the impact of sociodemographic factors on disease development, management, and outcomes in adult and pediatric populations. Given that postoperative management is key in reducing complications following a tracheotomy, we assessed the impact of sociodemographic factors on a patient's discharge disposition.</p><p><strong>Study design: </strong>Cross-sectional study.</p><p><strong>Setting: </strong>Health Care Utilization Project's (HCUP) National Inpatient Survey (NIS).</p><p><strong>Methods: </strong>The HCUP NIS was queried for all patients undergoing tracheotomy between 2017 and 2021. All analyses were performed using R Version 4.3.1 survey procedures to account for strata and cluster effects.</p><p><strong>Results: </strong>We identified 81,069 admissions during which a tracheotomy was performed and, after appropriate weighting for the HCUP NIS survey design, found that 15.1% of admissions resulted in routine discharge, 4.5% transferred to a short-term hospital, 52.3% transferred to a skilled nursing facility (SNF)/intermediate care facility (ICF)/other facility, 16.9% discharged with home health care. Admissions routinely discharged had the lowest median (interquartile range) age (48 [23, 61] years), whereas admissions resulting in death or transfer to a SNF/ICF/other facility type had the greatest age (63 [53, 70] years). On both univariable and multivariable analyses, age, race, sex, insurance type, geographic region, and hospital size were associated with discharge disposition.</p><p><strong>Conclusion: </strong>Our study highlights that disparities exist among patient populations and were found in both unadjusted and adjusted analyses. Further attention and resource allocation for the care of patients with a tracheostomy may work toward identifying sources of disparity, which may be modified to improve patient care.</p>\",\"PeriodicalId\":19697,\"journal\":{\"name\":\"OTO Open\",\"volume\":\"9 2\",\"pages\":\"e70129\"},\"PeriodicalIF\":1.8000,\"publicationDate\":\"2025-05-16\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12082083/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"OTO Open\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1002/oto2.70129\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/4/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"OTORHINOLARYNGOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"OTO Open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1002/oto2.70129","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/4/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"OTORHINOLARYNGOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
目的:以前的研究已经证明了社会人口因素对成人和儿童人群的疾病发展、管理和结局的影响。鉴于术后管理是减少气管切开术并发症的关键,我们评估了社会人口因素对患者出院处置的影响。研究设计:横断面研究。背景:卫生保健利用项目(HCUP)全国住院患者调查(NIS)。方法:对2017 - 2021年所有气管切开术患者的HCUP NIS进行查询。所有分析均使用R Version 4.3.1调查程序进行,以考虑地层和集群效应。结果:我们确定了81,069例接受气管切开术的入院患者,在对HCUP NIS调查设计进行适当加权后,发现15.1%的入院患者常规出院,4.5%转到短期医院,52.3%转到熟练护理机构(SNF)/中级护理机构(ICF)/其他机构,16.9%的患者出院时接受了家庭保健。常规出院的入院患者年龄中位数最低(四分位数范围)(48岁[23,61]),而入院导致死亡或转移到SNF/ICF/其他设施类型的患者年龄最大(63岁[53,70])。在单变量和多变量分析中,年龄、种族、性别、保险类型、地理区域和医院规模与出院处置有关。结论:我们的研究强调在患者群体中存在差异,并且在未调整和调整的分析中都发现了差异。对气管切开术患者护理的进一步关注和资源分配可能有助于确定差异的来源,从而改进患者护理。
Disparities in Posthospitalization Disposition Following Tracheotomy: A National Analysis.
Objective: Previous studies have demonstrated the impact of sociodemographic factors on disease development, management, and outcomes in adult and pediatric populations. Given that postoperative management is key in reducing complications following a tracheotomy, we assessed the impact of sociodemographic factors on a patient's discharge disposition.
Study design: Cross-sectional study.
Setting: Health Care Utilization Project's (HCUP) National Inpatient Survey (NIS).
Methods: The HCUP NIS was queried for all patients undergoing tracheotomy between 2017 and 2021. All analyses were performed using R Version 4.3.1 survey procedures to account for strata and cluster effects.
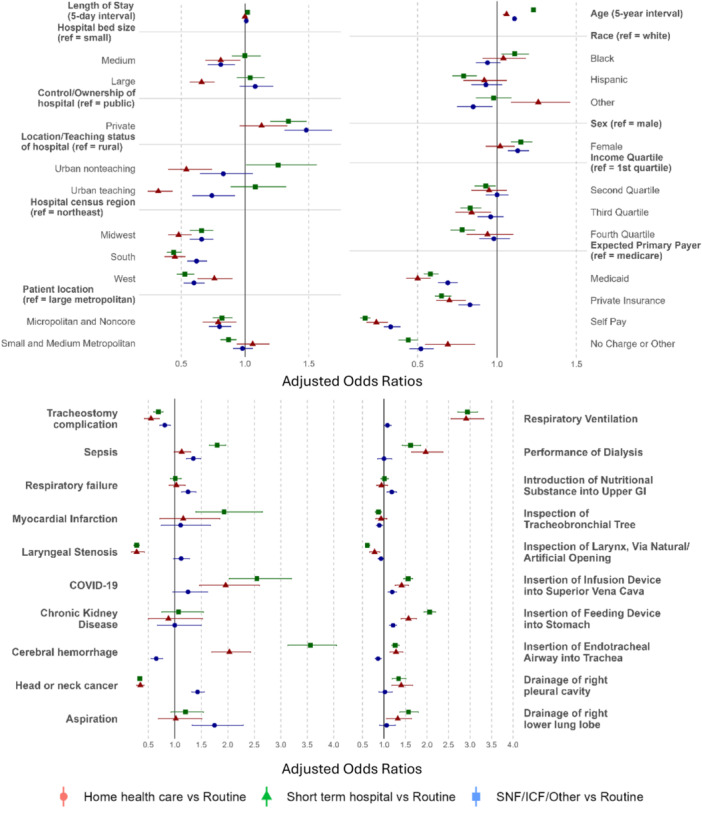
Results: We identified 81,069 admissions during which a tracheotomy was performed and, after appropriate weighting for the HCUP NIS survey design, found that 15.1% of admissions resulted in routine discharge, 4.5% transferred to a short-term hospital, 52.3% transferred to a skilled nursing facility (SNF)/intermediate care facility (ICF)/other facility, 16.9% discharged with home health care. Admissions routinely discharged had the lowest median (interquartile range) age (48 [23, 61] years), whereas admissions resulting in death or transfer to a SNF/ICF/other facility type had the greatest age (63 [53, 70] years). On both univariable and multivariable analyses, age, race, sex, insurance type, geographic region, and hospital size were associated with discharge disposition.
Conclusion: Our study highlights that disparities exist among patient populations and were found in both unadjusted and adjusted analyses. Further attention and resource allocation for the care of patients with a tracheostomy may work toward identifying sources of disparity, which may be modified to improve patient care.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:



