Johanne D Lyhne, Vibeke B Hansen, Lone D Vestergaard, Susanne E Hosbond, Martin Busk, Mayooran Gnanaganesh, Else Maae, Birgitte M Havelund, Torben F Hansen, Signe Timm, Lars H Jensen, Mads D Lyhne
{"title":"氟嘧啶治疗癌症患者心脏毒性的一级预防:一项随机对照试验","authors":"Johanne D Lyhne, Vibeke B Hansen, Lone D Vestergaard, Susanne E Hosbond, Martin Busk, Mayooran Gnanaganesh, Else Maae, Birgitte M Havelund, Torben F Hansen, Signe Timm, Lars H Jensen, Mads D Lyhne","doi":"10.1186/s40959-025-00344-3","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Fluoropyrimidines (FP) are the third most used chemotherapeutic drugs administered in solid tumors but have cardiotoxic side effects. We aimed to determine whether pre-chemotherapeutic cardiological assessment and management of cardiovascular risk factors could prevent FP-induced cardiotoxicity and if the coronary artery calcium (CAC) score was predictive of chest pain.</p><p><strong>Methods: </strong>This was a randomized, controlled, single center trial of patients with various cancer types who were treated with FP and had no known ischemic heart disease. All patients had CAC score obtained by cardiac CT scan. Patients were randomized to pre-chemotherapeutic cardiological management or standard care. Cardiological management included risk reduction based on electro- and echocardiographic evaluation and blood samples. Primary composite endpoint included hospital admission for chest pain, acute coronary syndrome, coronary angiography intervention, or all-cause mortality. Secondary outcome was chest pain. Follow-up was 6 months. Data were analyzed using Kaplan-Meier survival function with log-rank test and ROC-analyses.</p><p><strong>Results: </strong>Of the 192 patients included, the primary endpoint occurred in 9/95 (9.5%) patients in the intervention group and 15/97 (15.5%) patients in the control group (log-rank p = 0.19) with an incidence rate ratio (IRR) of 0.57 (95% CI [0.22 - 1.39]). Chest pain occurred in 6/95 (6.3%) patients in the intervention group and 13/97 (13.4%) in the control group, yielding an IRR of 0.44 (95% CI [0.14 - 1.23]). CAC score did not predict chest pain occurrence.</p><p><strong>Conclusions: </strong>Cardiological management of cardiovascular risk factors prior to treatment with fluoropyrimidines resulted in half as many cardiotoxic events but the study did not reach statistical significance. Further studies are needed to investigate the optimal strategies to prevent fluoropyrimidine-induced cardiotoxicity in cancer patients.</p><p><strong>Trial registration: </strong>ClinicalTrials.gov Identifyer NCT03486340.</p>","PeriodicalId":9804,"journal":{"name":"Cardio-oncology","volume":"11 1","pages":"48"},"PeriodicalIF":3.2000,"publicationDate":"2025-05-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12084922/pdf/","citationCount":"0","resultStr":"{\"title\":\"Primary prevention of cardiotoxicity in cancer patients treated with fluoropyrimidines: a randomized controlled trial.\",\"authors\":\"Johanne D Lyhne, Vibeke B Hansen, Lone D Vestergaard, Susanne E Hosbond, Martin Busk, Mayooran Gnanaganesh, Else Maae, Birgitte M Havelund, Torben F Hansen, Signe Timm, Lars H Jensen, Mads D Lyhne\",\"doi\":\"10.1186/s40959-025-00344-3\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Fluoropyrimidines (FP) are the third most used chemotherapeutic drugs administered in solid tumors but have cardiotoxic side effects. We aimed to determine whether pre-chemotherapeutic cardiological assessment and management of cardiovascular risk factors could prevent FP-induced cardiotoxicity and if the coronary artery calcium (CAC) score was predictive of chest pain.</p><p><strong>Methods: </strong>This was a randomized, controlled, single center trial of patients with various cancer types who were treated with FP and had no known ischemic heart disease. All patients had CAC score obtained by cardiac CT scan. Patients were randomized to pre-chemotherapeutic cardiological management or standard care. Cardiological management included risk reduction based on electro- and echocardiographic evaluation and blood samples. Primary composite endpoint included hospital admission for chest pain, acute coronary syndrome, coronary angiography intervention, or all-cause mortality. Secondary outcome was chest pain. Follow-up was 6 months. Data were analyzed using Kaplan-Meier survival function with log-rank test and ROC-analyses.</p><p><strong>Results: </strong>Of the 192 patients included, the primary endpoint occurred in 9/95 (9.5%) patients in the intervention group and 15/97 (15.5%) patients in the control group (log-rank p = 0.19) with an incidence rate ratio (IRR) of 0.57 (95% CI [0.22 - 1.39]). Chest pain occurred in 6/95 (6.3%) patients in the intervention group and 13/97 (13.4%) in the control group, yielding an IRR of 0.44 (95% CI [0.14 - 1.23]). CAC score did not predict chest pain occurrence.</p><p><strong>Conclusions: </strong>Cardiological management of cardiovascular risk factors prior to treatment with fluoropyrimidines resulted in half as many cardiotoxic events but the study did not reach statistical significance. Further studies are needed to investigate the optimal strategies to prevent fluoropyrimidine-induced cardiotoxicity in cancer patients.</p><p><strong>Trial registration: </strong>ClinicalTrials.gov Identifyer NCT03486340.</p>\",\"PeriodicalId\":9804,\"journal\":{\"name\":\"Cardio-oncology\",\"volume\":\"11 1\",\"pages\":\"48\"},\"PeriodicalIF\":3.2000,\"publicationDate\":\"2025-05-17\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12084922/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Cardio-oncology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/s40959-025-00344-3\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cardio-oncology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s40959-025-00344-3","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
Primary prevention of cardiotoxicity in cancer patients treated with fluoropyrimidines: a randomized controlled trial.
Background: Fluoropyrimidines (FP) are the third most used chemotherapeutic drugs administered in solid tumors but have cardiotoxic side effects. We aimed to determine whether pre-chemotherapeutic cardiological assessment and management of cardiovascular risk factors could prevent FP-induced cardiotoxicity and if the coronary artery calcium (CAC) score was predictive of chest pain.
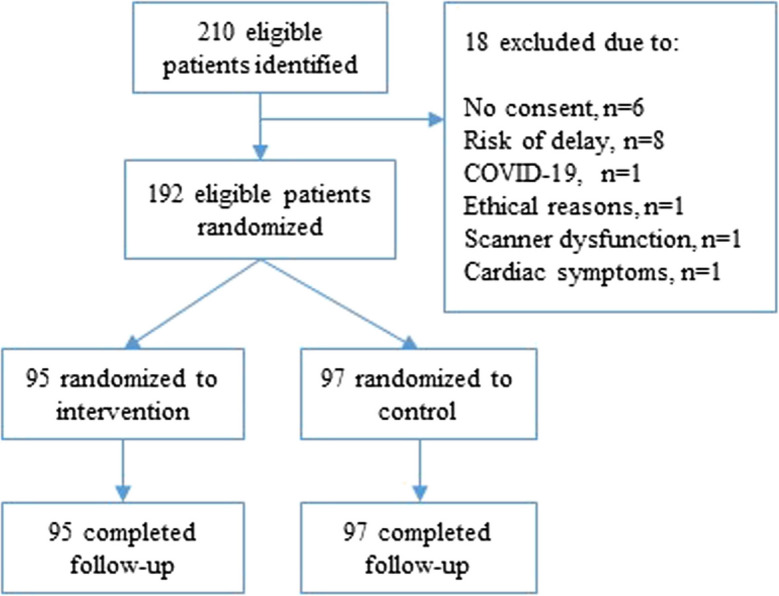
Methods: This was a randomized, controlled, single center trial of patients with various cancer types who were treated with FP and had no known ischemic heart disease. All patients had CAC score obtained by cardiac CT scan. Patients were randomized to pre-chemotherapeutic cardiological management or standard care. Cardiological management included risk reduction based on electro- and echocardiographic evaluation and blood samples. Primary composite endpoint included hospital admission for chest pain, acute coronary syndrome, coronary angiography intervention, or all-cause mortality. Secondary outcome was chest pain. Follow-up was 6 months. Data were analyzed using Kaplan-Meier survival function with log-rank test and ROC-analyses.
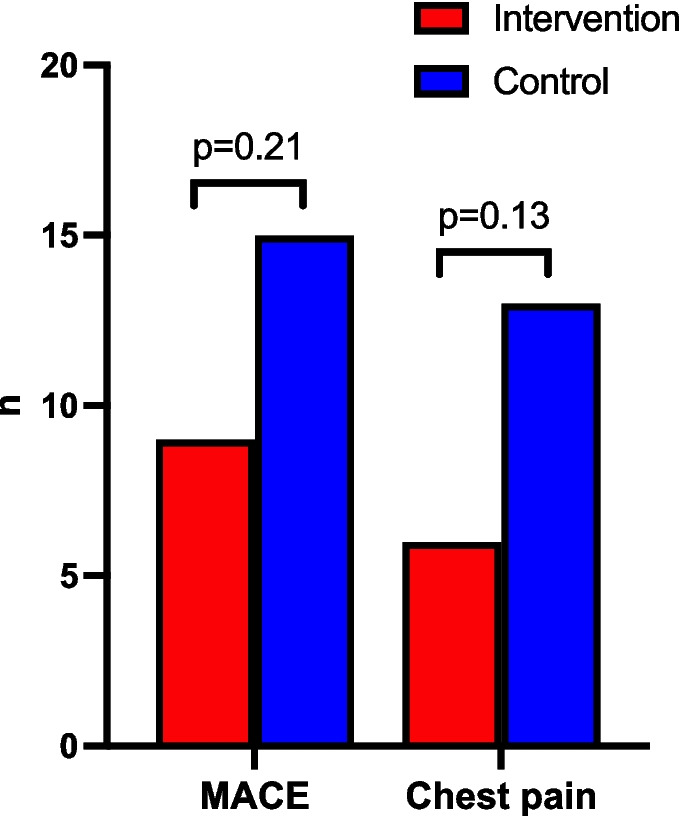
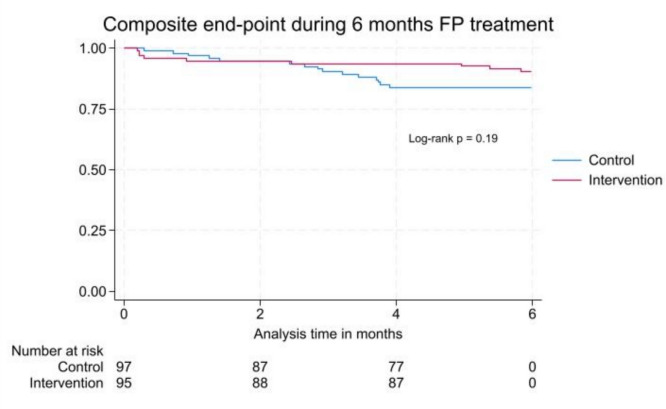
Results: Of the 192 patients included, the primary endpoint occurred in 9/95 (9.5%) patients in the intervention group and 15/97 (15.5%) patients in the control group (log-rank p = 0.19) with an incidence rate ratio (IRR) of 0.57 (95% CI [0.22 - 1.39]). Chest pain occurred in 6/95 (6.3%) patients in the intervention group and 13/97 (13.4%) in the control group, yielding an IRR of 0.44 (95% CI [0.14 - 1.23]). CAC score did not predict chest pain occurrence.
Conclusions: Cardiological management of cardiovascular risk factors prior to treatment with fluoropyrimidines resulted in half as many cardiotoxic events but the study did not reach statistical significance. Further studies are needed to investigate the optimal strategies to prevent fluoropyrimidine-induced cardiotoxicity in cancer patients.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


