Anthony J Weekes, Fernanda Calienescerpa, Kelly L Goonan, Alexa L Polzella, Melanie M Hogg, Dalton Cox, Sean Flannigan, Emma Cruz, Halie A O'Neill, Nathaniel S O'Connell, Daniel R Troha
{"title":"国家早期预警评分与肺栓塞临床恶化的关系。","authors":"Anthony J Weekes, Fernanda Calienescerpa, Kelly L Goonan, Alexa L Polzella, Melanie M Hogg, Dalton Cox, Sean Flannigan, Emma Cruz, Halie A O'Neill, Nathaniel S O'Connell, Daniel R Troha","doi":"10.1186/s12959-025-00735-7","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The National Early Warning Score (NEWS2) predicts clinical deterioration in hospitalized patients. Its role in pulmonary embolism (PE) risk stratification remains underexplored. This study assessed the association of initial NEWS2 with clinical deterioration and advanced interventions during hospitalization.</p><p><strong>Methods: </strong>We retrospectively analyzed a PE response team (PERT) registry of adults with submassive and massive PE from 11 emergency departments (2016-2024). Initial NEWS2 was calculated for each registry patient. The primary outcome was in-hospital PE-related clinical deterioration (death, cardiac arrest, vasoactive medications for hypotension, or emergent respiratory interventions). The secondary outcome was advanced intervention use. We calculated odds ratios (OR) for different NEWS2 cut-offs. We used multivariable analysis to assess the association of NEWS2 and study outcomes, and decision curve analysis to determine net benefit of clinical deterioration.</p><p><strong>Results: </strong>Among 2119 patients (mean age 62.2 [16.8], 51.2% female, 168 [7.9%] with massive PE, and 1951 [92.1%] with submassive PE), 309 patients (14.6%) experienced clinical deterioration and 488 (23.0%) required advanced interventions. Mean NEWS2 was higher in patients with vs. without clinical deterioration (6.0 ± 3.3 vs. 3.0 ± 2.4; p < 0.001) and in those with vs. without advanced interventions (4.8 ± 3.1 vs. 3.0 ± 2.5; p < 0.001). NEWS2 cut-off of ≥ 3 identified patients at risk of clinical deterioration: sensitivity 87% (82-90%), OR 6.1 (95% CI: 4.3-8.5), and negative predictive value (NPV) 96% (94-97%). NEWS2 cut-off ≥ 4 had specificity of 62% (60-65%), OR of 5.1 (95% CI: 3.9-6.7), and NPV of 94% (92-95%). As a continuous variable, NEWS2 had an OR of 1.2 (95% CI: 1.1-1.3). NEWS2 cut-offs from 3 to 5 showed an improved net benefit (0.08, 0.16, and 0.34) compared with treating all patients as high risk for clinical deterioration.</p><p><strong>Conclusion: </strong>Patients with PE and initial NEWS2 scores ≥ 3 had a four-fold to eight-fold higher odds of clinical deterioration than those with NEWS2 < 3. NEWS2 is useful for predicting clinical deterioration and guiding intervention strategies in PE.</p>","PeriodicalId":22982,"journal":{"name":"Thrombosis Journal","volume":"23 1","pages":"49"},"PeriodicalIF":2.2000,"publicationDate":"2025-05-16","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12083166/pdf/","citationCount":"0","resultStr":"{\"title\":\"Association of initial national early warning score with clinical deterioration in pulmonary embolism.\",\"authors\":\"Anthony J Weekes, Fernanda Calienescerpa, Kelly L Goonan, Alexa L Polzella, Melanie M Hogg, Dalton Cox, Sean Flannigan, Emma Cruz, Halie A O'Neill, Nathaniel S O'Connell, Daniel R Troha\",\"doi\":\"10.1186/s12959-025-00735-7\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>The National Early Warning Score (NEWS2) predicts clinical deterioration in hospitalized patients. Its role in pulmonary embolism (PE) risk stratification remains underexplored. This study assessed the association of initial NEWS2 with clinical deterioration and advanced interventions during hospitalization.</p><p><strong>Methods: </strong>We retrospectively analyzed a PE response team (PERT) registry of adults with submassive and massive PE from 11 emergency departments (2016-2024). Initial NEWS2 was calculated for each registry patient. The primary outcome was in-hospital PE-related clinical deterioration (death, cardiac arrest, vasoactive medications for hypotension, or emergent respiratory interventions). The secondary outcome was advanced intervention use. We calculated odds ratios (OR) for different NEWS2 cut-offs. We used multivariable analysis to assess the association of NEWS2 and study outcomes, and decision curve analysis to determine net benefit of clinical deterioration.</p><p><strong>Results: </strong>Among 2119 patients (mean age 62.2 [16.8], 51.2% female, 168 [7.9%] with massive PE, and 1951 [92.1%] with submassive PE), 309 patients (14.6%) experienced clinical deterioration and 488 (23.0%) required advanced interventions. Mean NEWS2 was higher in patients with vs. without clinical deterioration (6.0 ± 3.3 vs. 3.0 ± 2.4; p < 0.001) and in those with vs. without advanced interventions (4.8 ± 3.1 vs. 3.0 ± 2.5; p < 0.001). NEWS2 cut-off of ≥ 3 identified patients at risk of clinical deterioration: sensitivity 87% (82-90%), OR 6.1 (95% CI: 4.3-8.5), and negative predictive value (NPV) 96% (94-97%). NEWS2 cut-off ≥ 4 had specificity of 62% (60-65%), OR of 5.1 (95% CI: 3.9-6.7), and NPV of 94% (92-95%). As a continuous variable, NEWS2 had an OR of 1.2 (95% CI: 1.1-1.3). NEWS2 cut-offs from 3 to 5 showed an improved net benefit (0.08, 0.16, and 0.34) compared with treating all patients as high risk for clinical deterioration.</p><p><strong>Conclusion: </strong>Patients with PE and initial NEWS2 scores ≥ 3 had a four-fold to eight-fold higher odds of clinical deterioration than those with NEWS2 < 3. NEWS2 is useful for predicting clinical deterioration and guiding intervention strategies in PE.</p>\",\"PeriodicalId\":22982,\"journal\":{\"name\":\"Thrombosis Journal\",\"volume\":\"23 1\",\"pages\":\"49\"},\"PeriodicalIF\":2.2000,\"publicationDate\":\"2025-05-16\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12083166/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Thrombosis Journal\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1186/s12959-025-00735-7\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"HEMATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Thrombosis Journal","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s12959-025-00735-7","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"HEMATOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
背景:国家早期预警评分(NEWS2)预测住院患者的临床恶化。它在肺栓塞(PE)风险分层中的作用仍未得到充分探讨。本研究评估了初始NEWS2与住院期间临床恶化和晚期干预的关系。方法:我们回顾性分析了来自11个急诊科(2016-2024年)的PE反应小组(PERT)登记的成人亚肿块和巨大PE。计算每个注册患者的初始NEWS2。主要结局是院内pe相关的临床恶化(死亡、心脏骤停、血管活性降压药物或紧急呼吸干预)。次要结果是晚期干预措施的使用。我们计算了不同NEWS2截止点的比值比(OR)。我们使用多变量分析来评估NEWS2与研究结果的关联,并使用决策曲线分析来确定临床恶化的净收益。结果:2119例患者(平均年龄62.2岁[16.8],女性51.2%,块状PE 168例[7.9%],次块状PE 1951例[92.1%])中,309例(14.6%)出现临床恶化,488例(23.0%)需要进行晚期干预。有临床恶化的患者的平均NEWS2高于无临床恶化的患者(6.0±3.3 vs 3.0±2.4;结论:PE和初始NEWS2评分≥3的患者临床恶化的几率比NEWS2患者高4 - 8倍
Association of initial national early warning score with clinical deterioration in pulmonary embolism.
Background: The National Early Warning Score (NEWS2) predicts clinical deterioration in hospitalized patients. Its role in pulmonary embolism (PE) risk stratification remains underexplored. This study assessed the association of initial NEWS2 with clinical deterioration and advanced interventions during hospitalization.
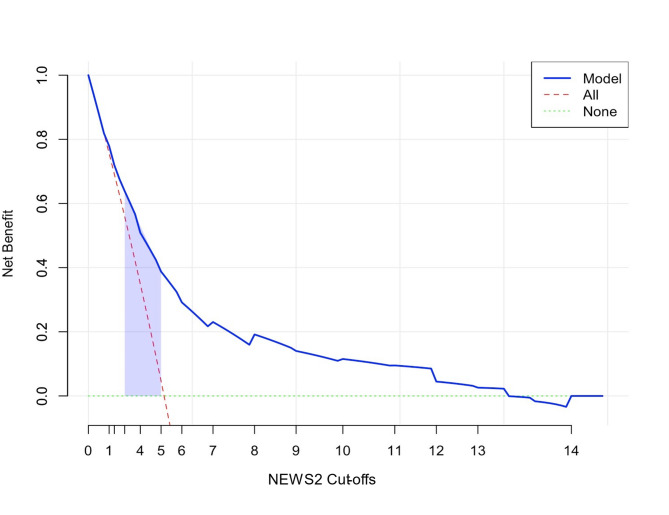
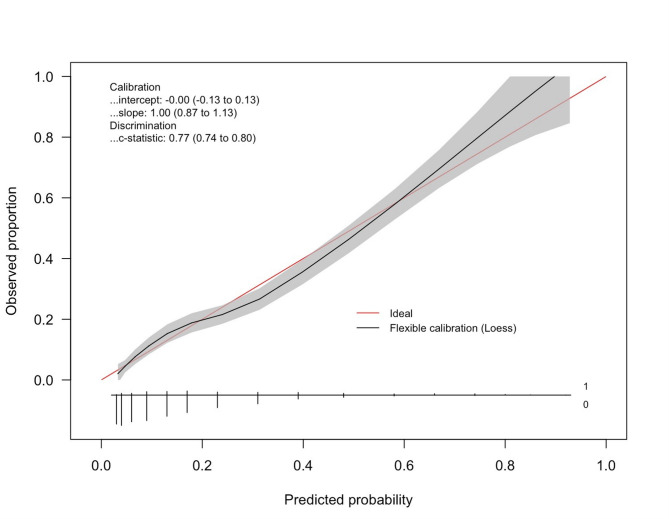
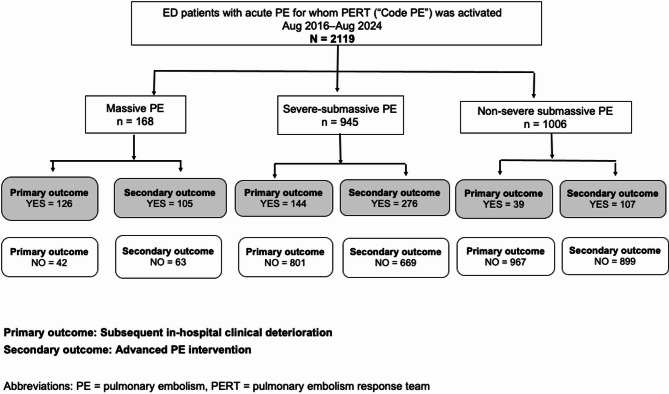
Methods: We retrospectively analyzed a PE response team (PERT) registry of adults with submassive and massive PE from 11 emergency departments (2016-2024). Initial NEWS2 was calculated for each registry patient. The primary outcome was in-hospital PE-related clinical deterioration (death, cardiac arrest, vasoactive medications for hypotension, or emergent respiratory interventions). The secondary outcome was advanced intervention use. We calculated odds ratios (OR) for different NEWS2 cut-offs. We used multivariable analysis to assess the association of NEWS2 and study outcomes, and decision curve analysis to determine net benefit of clinical deterioration.
Results: Among 2119 patients (mean age 62.2 [16.8], 51.2% female, 168 [7.9%] with massive PE, and 1951 [92.1%] with submassive PE), 309 patients (14.6%) experienced clinical deterioration and 488 (23.0%) required advanced interventions. Mean NEWS2 was higher in patients with vs. without clinical deterioration (6.0 ± 3.3 vs. 3.0 ± 2.4; p < 0.001) and in those with vs. without advanced interventions (4.8 ± 3.1 vs. 3.0 ± 2.5; p < 0.001). NEWS2 cut-off of ≥ 3 identified patients at risk of clinical deterioration: sensitivity 87% (82-90%), OR 6.1 (95% CI: 4.3-8.5), and negative predictive value (NPV) 96% (94-97%). NEWS2 cut-off ≥ 4 had specificity of 62% (60-65%), OR of 5.1 (95% CI: 3.9-6.7), and NPV of 94% (92-95%). As a continuous variable, NEWS2 had an OR of 1.2 (95% CI: 1.1-1.3). NEWS2 cut-offs from 3 to 5 showed an improved net benefit (0.08, 0.16, and 0.34) compared with treating all patients as high risk for clinical deterioration.
Conclusion: Patients with PE and initial NEWS2 scores ≥ 3 had a four-fold to eight-fold higher odds of clinical deterioration than those with NEWS2 < 3. NEWS2 is useful for predicting clinical deterioration and guiding intervention strategies in PE.
期刊介绍:
Thrombosis Journal is an open-access journal that publishes original articles on aspects of clinical and basic research, new methodology, case reports and reviews in the areas of thrombosis.
Topics of particular interest include the diagnosis of arterial and venous thrombosis, new antithrombotic treatments, new developments in the understanding, diagnosis and treatments of atherosclerotic vessel disease, relations between haemostasis and vascular disease, hypertension, diabetes, immunology and obesity.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


