Asem Ali Ashraf, Sayantani Nag, Vimal Kumar Karnaker
{"title":"继发性自发性气胸并发罕见粘质沙雷菌胸膜感染1例。","authors":"Asem Ali Ashraf, Sayantani Nag, Vimal Kumar Karnaker","doi":"10.12701/jyms.2025.42.35","DOIUrl":null,"url":null,"abstract":"<p><p>Serratia marcescens is an opportunistic gram-negative pathogen that causes pneumonia, bloodstream infections, and urinary tract infections, particularly in individuals who are immunocompromised. Although commonly associated with pulmonary infections, its involvement in pneumothorax-related infections is exceedingly rare. Secondary spontaneous pneumothorax (SSP) is a life-threatening condition that can complicate underlying lung diseases, such as chronic obstructive pulmonary disease (COPD). This case report describes a rare presentation of S. marcescens infection in a patient with SSP complicated by a bronchopleural fistula. A 64-year-old male with a history of COPD, chronic smoking, and alcohol use presented with progressive dyspnea, cough, and left-sided chest pain. Clinical evaluation revealed tachypnea, tracheal deviation, and reduced breath sounds in the left lung. Laboratory investigations revealed leukocytosis with marked neutrophilia and an elevated erythrocyte sedimentation rate. Chest imaging confirmed pneumothorax, necessitating intercostal drain (ICD) placement. Pleural fluid cultures identified multidrug-resistant S. marcescens, prompting antibiotic escalation to intravenous meropenem and oral faropenem. Despite prolonged antimicrobial therapy and ICD placement, persistent pneumothorax with a bronchopleural fistula was noted. Bronchoscopy with Fogarty balloon placement and cyanoacrylate closure was performed. However, owing to financial constraints, the patient declined follow-up cultures and high-resolution computed tomography imaging, and was discharged with an ICD in situ. This case underscores the need for heightened clinical awareness of S. marcescens in pneumothorax-associated infections. Early microbiological identification and targeted therapy are crucial for the management of rare yet challenging presentations, particularly in resource-limited settings.</p>","PeriodicalId":74020,"journal":{"name":"Journal of Yeungnam medical science","volume":"42 ","pages":"35"},"PeriodicalIF":1.4000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12303781/pdf/","citationCount":"0","resultStr":"{\"title\":\"Unusual Serratia marcescens pleural infection in secondary spontaneous pneumothorax: a case report.\",\"authors\":\"Asem Ali Ashraf, Sayantani Nag, Vimal Kumar Karnaker\",\"doi\":\"10.12701/jyms.2025.42.35\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Serratia marcescens is an opportunistic gram-negative pathogen that causes pneumonia, bloodstream infections, and urinary tract infections, particularly in individuals who are immunocompromised. Although commonly associated with pulmonary infections, its involvement in pneumothorax-related infections is exceedingly rare. Secondary spontaneous pneumothorax (SSP) is a life-threatening condition that can complicate underlying lung diseases, such as chronic obstructive pulmonary disease (COPD). This case report describes a rare presentation of S. marcescens infection in a patient with SSP complicated by a bronchopleural fistula. A 64-year-old male with a history of COPD, chronic smoking, and alcohol use presented with progressive dyspnea, cough, and left-sided chest pain. Clinical evaluation revealed tachypnea, tracheal deviation, and reduced breath sounds in the left lung. Laboratory investigations revealed leukocytosis with marked neutrophilia and an elevated erythrocyte sedimentation rate. Chest imaging confirmed pneumothorax, necessitating intercostal drain (ICD) placement. Pleural fluid cultures identified multidrug-resistant S. marcescens, prompting antibiotic escalation to intravenous meropenem and oral faropenem. Despite prolonged antimicrobial therapy and ICD placement, persistent pneumothorax with a bronchopleural fistula was noted. Bronchoscopy with Fogarty balloon placement and cyanoacrylate closure was performed. However, owing to financial constraints, the patient declined follow-up cultures and high-resolution computed tomography imaging, and was discharged with an ICD in situ. This case underscores the need for heightened clinical awareness of S. marcescens in pneumothorax-associated infections. Early microbiological identification and targeted therapy are crucial for the management of rare yet challenging presentations, particularly in resource-limited settings.</p>\",\"PeriodicalId\":74020,\"journal\":{\"name\":\"Journal of Yeungnam medical science\",\"volume\":\"42 \",\"pages\":\"35\"},\"PeriodicalIF\":1.4000,\"publicationDate\":\"2025-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12303781/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Yeungnam medical science\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.12701/jyms.2025.42.35\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/5/15 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"MEDICINE, GENERAL & INTERNAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Yeungnam medical science","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.12701/jyms.2025.42.35","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/5/15 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
Unusual Serratia marcescens pleural infection in secondary spontaneous pneumothorax: a case report.
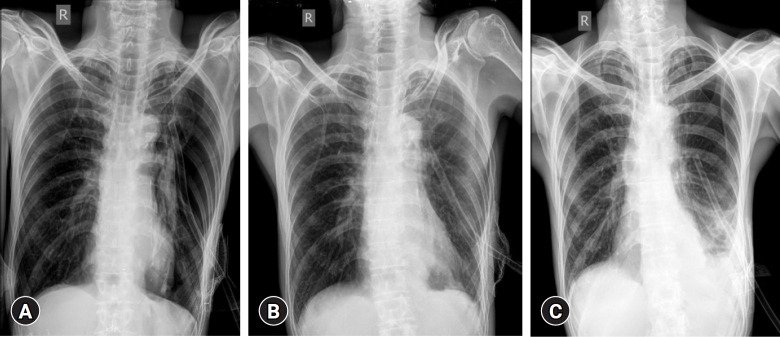
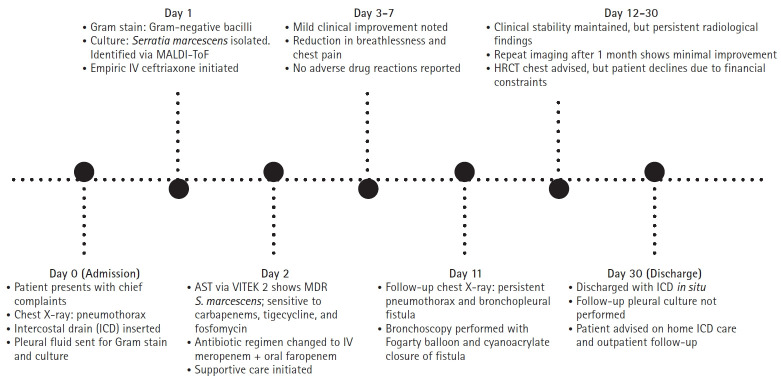
Serratia marcescens is an opportunistic gram-negative pathogen that causes pneumonia, bloodstream infections, and urinary tract infections, particularly in individuals who are immunocompromised. Although commonly associated with pulmonary infections, its involvement in pneumothorax-related infections is exceedingly rare. Secondary spontaneous pneumothorax (SSP) is a life-threatening condition that can complicate underlying lung diseases, such as chronic obstructive pulmonary disease (COPD). This case report describes a rare presentation of S. marcescens infection in a patient with SSP complicated by a bronchopleural fistula. A 64-year-old male with a history of COPD, chronic smoking, and alcohol use presented with progressive dyspnea, cough, and left-sided chest pain. Clinical evaluation revealed tachypnea, tracheal deviation, and reduced breath sounds in the left lung. Laboratory investigations revealed leukocytosis with marked neutrophilia and an elevated erythrocyte sedimentation rate. Chest imaging confirmed pneumothorax, necessitating intercostal drain (ICD) placement. Pleural fluid cultures identified multidrug-resistant S. marcescens, prompting antibiotic escalation to intravenous meropenem and oral faropenem. Despite prolonged antimicrobial therapy and ICD placement, persistent pneumothorax with a bronchopleural fistula was noted. Bronchoscopy with Fogarty balloon placement and cyanoacrylate closure was performed. However, owing to financial constraints, the patient declined follow-up cultures and high-resolution computed tomography imaging, and was discharged with an ICD in situ. This case underscores the need for heightened clinical awareness of S. marcescens in pneumothorax-associated infections. Early microbiological identification and targeted therapy are crucial for the management of rare yet challenging presentations, particularly in resource-limited settings.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


