Thamires de Carvalho Silvério, Cristiane do Prado, Milena Siciliano Nascimento
{"title":"拔管失败对儿童机械通气持续时间的影响。","authors":"Thamires de Carvalho Silvério, Cristiane do Prado, Milena Siciliano Nascimento","doi":"10.31744/einstein_journal/2025AO0705","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The study demonstrated that extubation failure prolonged the total duration of mechanical ventilation to twice that observed in patients with successful extubation. These findings emphasize the critical need for daily patient assessment guided by well-defined clinical criteria to ensure mechanical ventilation is discontinued precisely when the patient is clinically prepared-neither prematurely nor unnecessarily delayed. ■ In patients who experienced extubation failure, the total ventilation time was twice as long as that of patients with successful extubation. ■ The incidence of extubation failure was 5.2%, which is relatively low compared to other studies. ■ The study revealed no significant association between the presence of pre-existing illnesses and extubation outcomes. ■ Results indicated that the primary cause of extubation failure was upper airway obstruction, accounting for 67% of cases requiring reintubation.</p><p><strong>Objective: </strong>To compare the epidemiological profiles of patients who experienced extubation failure with those who achieved success and to evaluate the impact of extubation failure on total mechanical ventilation duration.</p><p><strong>Methods: </strong>An observational study with both retrospective and prospective components was conducted on patients admitted to the Pediatric Intensive Care Unit of a private hospital. This study included patients who underwent mechanical ventilation and were extubated between January 2017 and December 2022. Patients were classified into extubation Success or Failure Groups, with failure defined as requiring a return to invasive mechanical ventilation within 48hs post-extubation. Epidemiological factors, including age, pre-existing illnesses, and time on invasive mechanical ventilation, were analyzed.</p><p><strong>Results: </strong>A total of 173 patients were included, of which 9 (5.2%) required reintubation within 48hs. The total duration of mechanical ventilation differed significantly between the Success Group (3 days [1.8; 6.6]) and the Failure Group (6.5 days [5.6; 9.3]), p=0.004. Upper airway obstruction was identified as the primary cause of extubation failure.</p><p><strong>Conclusion: </strong>This study demonstrated that extubation failure doubled the total duration of mechanical ventilation compared to successful extubation. These findings highlight the importance of daily patient assessment with clearly defined clinical criteria to ensure mechanical ventilation is discontinued precisely when the patient is ready-neither prematurely nor excessively delayed.</p>","PeriodicalId":47359,"journal":{"name":"Einstein-Sao Paulo","volume":"23 ","pages":"eAO0705"},"PeriodicalIF":0.9000,"publicationDate":"2025-05-12","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12094675/pdf/","citationCount":"0","resultStr":"{\"title\":\"Impact of extubation failure on the duration of mechanical ventilation in the pediatric population.\",\"authors\":\"Thamires de Carvalho Silvério, Cristiane do Prado, Milena Siciliano Nascimento\",\"doi\":\"10.31744/einstein_journal/2025AO0705\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>The study demonstrated that extubation failure prolonged the total duration of mechanical ventilation to twice that observed in patients with successful extubation. These findings emphasize the critical need for daily patient assessment guided by well-defined clinical criteria to ensure mechanical ventilation is discontinued precisely when the patient is clinically prepared-neither prematurely nor unnecessarily delayed. ■ In patients who experienced extubation failure, the total ventilation time was twice as long as that of patients with successful extubation. ■ The incidence of extubation failure was 5.2%, which is relatively low compared to other studies. ■ The study revealed no significant association between the presence of pre-existing illnesses and extubation outcomes. ■ Results indicated that the primary cause of extubation failure was upper airway obstruction, accounting for 67% of cases requiring reintubation.</p><p><strong>Objective: </strong>To compare the epidemiological profiles of patients who experienced extubation failure with those who achieved success and to evaluate the impact of extubation failure on total mechanical ventilation duration.</p><p><strong>Methods: </strong>An observational study with both retrospective and prospective components was conducted on patients admitted to the Pediatric Intensive Care Unit of a private hospital. This study included patients who underwent mechanical ventilation and were extubated between January 2017 and December 2022. Patients were classified into extubation Success or Failure Groups, with failure defined as requiring a return to invasive mechanical ventilation within 48hs post-extubation. Epidemiological factors, including age, pre-existing illnesses, and time on invasive mechanical ventilation, were analyzed.</p><p><strong>Results: </strong>A total of 173 patients were included, of which 9 (5.2%) required reintubation within 48hs. The total duration of mechanical ventilation differed significantly between the Success Group (3 days [1.8; 6.6]) and the Failure Group (6.5 days [5.6; 9.3]), p=0.004. Upper airway obstruction was identified as the primary cause of extubation failure.</p><p><strong>Conclusion: </strong>This study demonstrated that extubation failure doubled the total duration of mechanical ventilation compared to successful extubation. These findings highlight the importance of daily patient assessment with clearly defined clinical criteria to ensure mechanical ventilation is discontinued precisely when the patient is ready-neither prematurely nor excessively delayed.</p>\",\"PeriodicalId\":47359,\"journal\":{\"name\":\"Einstein-Sao Paulo\",\"volume\":\"23 \",\"pages\":\"eAO0705\"},\"PeriodicalIF\":0.9000,\"publicationDate\":\"2025-05-12\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12094675/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Einstein-Sao Paulo\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.31744/einstein_journal/2025AO0705\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"MEDICINE, GENERAL & INTERNAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Einstein-Sao Paulo","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.31744/einstein_journal/2025AO0705","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
摘要
背景:本研究表明拔管失败使机械通气总时间延长至拔管成功患者的两倍。这些发现强调了在明确的临床标准指导下对患者进行日常评估的迫切需要,以确保在患者临床准备时精确地停止机械通气-既不过早也不不必要地延迟。■拔管失败患者的总通气时间是拔管成功患者的两倍。■拔管失败发生率为5.2%,与其他研究相比相对较低。■该研究显示,已有疾病的存在与拔管结果之间没有显著关联。■结果显示拔管失败的主要原因是上气道阻塞,占需要重新插管病例的67%。目的:比较拔管失败患者与成功拔管患者的流行病学特征,评价拔管失败对全机械通气时间的影响。方法:对一家私立医院儿科重症监护室收治的患者进行回顾性和前瞻性观察性研究。该研究包括2017年1月至2022年12月期间接受机械通气并拔管的患者。将患者分为拔管成功组和拔管失败组,拔管失败定义为拔管后48h内需要恢复有创机械通气。分析流行病学因素,包括年龄、既往疾病和有创机械通气时间。结果:共纳入173例患者,其中9例(5.2%)在48h内需要再插管。机械通气总持续时间在成功组(3天[1.8;6.6])和故障组(6.5天[5.6;9.3]), p = 0.004。上气道阻塞被确定为拔管失败的主要原因。结论:本研究表明拔管失败使机械通气总时间比拔管成功增加一倍。这些发现强调了每天对患者进行评估的重要性,明确了临床标准,以确保在患者准备就绪时准确停止机械通气——既不过早也不过度延迟。
Impact of extubation failure on the duration of mechanical ventilation in the pediatric population.
Background: The study demonstrated that extubation failure prolonged the total duration of mechanical ventilation to twice that observed in patients with successful extubation. These findings emphasize the critical need for daily patient assessment guided by well-defined clinical criteria to ensure mechanical ventilation is discontinued precisely when the patient is clinically prepared-neither prematurely nor unnecessarily delayed. ■ In patients who experienced extubation failure, the total ventilation time was twice as long as that of patients with successful extubation. ■ The incidence of extubation failure was 5.2%, which is relatively low compared to other studies. ■ The study revealed no significant association between the presence of pre-existing illnesses and extubation outcomes. ■ Results indicated that the primary cause of extubation failure was upper airway obstruction, accounting for 67% of cases requiring reintubation.
Objective: To compare the epidemiological profiles of patients who experienced extubation failure with those who achieved success and to evaluate the impact of extubation failure on total mechanical ventilation duration.
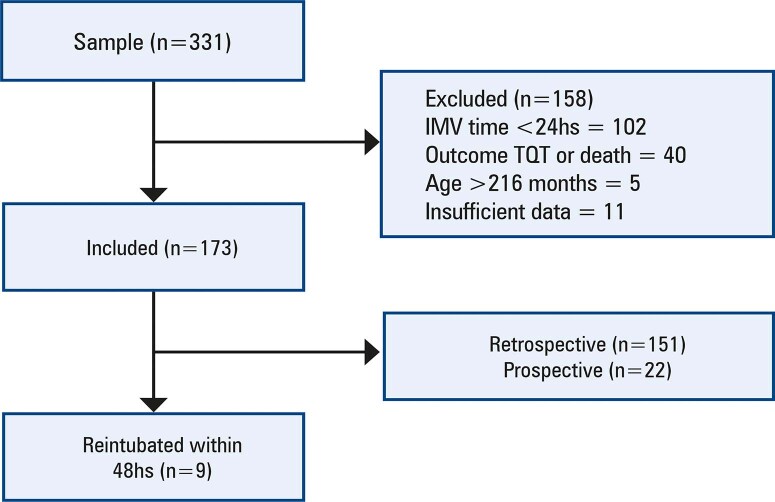
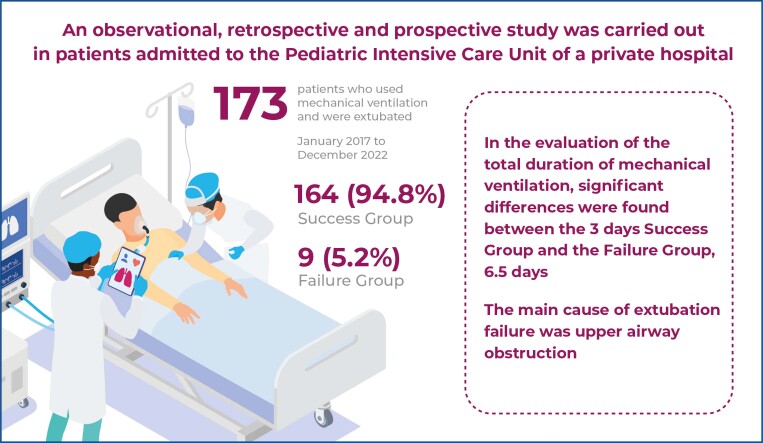
Methods: An observational study with both retrospective and prospective components was conducted on patients admitted to the Pediatric Intensive Care Unit of a private hospital. This study included patients who underwent mechanical ventilation and were extubated between January 2017 and December 2022. Patients were classified into extubation Success or Failure Groups, with failure defined as requiring a return to invasive mechanical ventilation within 48hs post-extubation. Epidemiological factors, including age, pre-existing illnesses, and time on invasive mechanical ventilation, were analyzed.
Results: A total of 173 patients were included, of which 9 (5.2%) required reintubation within 48hs. The total duration of mechanical ventilation differed significantly between the Success Group (3 days [1.8; 6.6]) and the Failure Group (6.5 days [5.6; 9.3]), p=0.004. Upper airway obstruction was identified as the primary cause of extubation failure.
Conclusion: This study demonstrated that extubation failure doubled the total duration of mechanical ventilation compared to successful extubation. These findings highlight the importance of daily patient assessment with clearly defined clinical criteria to ensure mechanical ventilation is discontinued precisely when the patient is ready-neither prematurely nor excessively delayed.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


