{"title":"重症监护病房患者中抗菌素潜在药物-药物相互作用的患病率和临床意义:一项回顾性研究。","authors":"Shanshan Xu, Zhihui Song, Jie Bai, Jiawei Wang","doi":"10.1186/s40360-025-00925-z","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Antimicrobials are frequently prescribed in Intensive Care Units (ICUs), where drug-drug interactions (DDIs) with other medications may exacerbate clinical outcomes. Limited evidence exists on the prevalence and clinical impact of these interactions.</p><p><strong>Objective: </strong>To estimate the prevalence of potential DDIs (pDDIs) between antimicrobials and other drugs in ICU patients using two electronic DDIs databases, identify the actual DDIs and the most frequently implicated antimicrobials, and determine the risk factors associated with actual DDIs.</p><p><strong>Methods: </strong>We conducted a retrospective study on patients admitted to intensive care units from January to December 2023. Micromedex and Lexi-Interact were used to identify pDDIs and their severities. Furthermore, we used the Drug Interaction Probability Scale (DIPS) criteria to identify actual DDIs.</p><p><strong>Results: </strong>Among 2,154 patients, 2,163 pDDIs (108 unique pairs) were identified in 461 patients, and 2.87% (62 pDDIs in 46 patients) were classified as actual DDIs. The antimicrobials most likely to cause pDDIs included quinolones, triazole antifungals, and linezolid. Antimicrobial-drug pairs with a higher incidence of severe pDDIs included linezolid-dopamine/metoclopramide (hypertension), voriconazole-budesonide for inhalation (increased serum concentration of budesonide), and levofloxacin-amiodarone (QT prolongation). The antimicrobial-drug pairs with a higher occurrence of actual DDIs included linezolid-dopamine/dobutamine (hypertension), fluconazole-amiodarone/ritonavir (QT prolongation), and cefoperazone/vancomycin-furosemide (nephrotoxicity). Moderate agreement existed between the two databases for pDDIs detection (Cohen's kappa = 0.546), but severity ratings diverged. Multivariable analysis identified the number of drugs per patient (OR = 1.178, p < 0.001), the number of antimicrobials per patient (OR = 1.146, p < 0.038), and the length of stay in the ICU (OR = 1.093, p < 0.038) as significant risk factors.</p><p><strong>Conclusions: </strong>High pDDI rates involving antimicrobials were observed in ICU patients, though actual DDIs were infrequent. Notable severe risk pairs warrant vigilant monitoring, especially with a higher occurrence of actual DDIs. Discrepancies in DDI databases emphasize the need for multi-tool validation to optimize medication safety.</p>","PeriodicalId":9023,"journal":{"name":"BMC Pharmacology & Toxicology","volume":"26 1","pages":"104"},"PeriodicalIF":2.7000,"publicationDate":"2025-05-14","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12076841/pdf/","citationCount":"0","resultStr":"{\"title\":\"Prevalence and clinical significance of potential drug-drug interactions of antimicrobials in Intensive Care Unit patients: a retrospective study.\",\"authors\":\"Shanshan Xu, Zhihui Song, Jie Bai, Jiawei Wang\",\"doi\":\"10.1186/s40360-025-00925-z\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Antimicrobials are frequently prescribed in Intensive Care Units (ICUs), where drug-drug interactions (DDIs) with other medications may exacerbate clinical outcomes. Limited evidence exists on the prevalence and clinical impact of these interactions.</p><p><strong>Objective: </strong>To estimate the prevalence of potential DDIs (pDDIs) between antimicrobials and other drugs in ICU patients using two electronic DDIs databases, identify the actual DDIs and the most frequently implicated antimicrobials, and determine the risk factors associated with actual DDIs.</p><p><strong>Methods: </strong>We conducted a retrospective study on patients admitted to intensive care units from January to December 2023. Micromedex and Lexi-Interact were used to identify pDDIs and their severities. Furthermore, we used the Drug Interaction Probability Scale (DIPS) criteria to identify actual DDIs.</p><p><strong>Results: </strong>Among 2,154 patients, 2,163 pDDIs (108 unique pairs) were identified in 461 patients, and 2.87% (62 pDDIs in 46 patients) were classified as actual DDIs. The antimicrobials most likely to cause pDDIs included quinolones, triazole antifungals, and linezolid. Antimicrobial-drug pairs with a higher incidence of severe pDDIs included linezolid-dopamine/metoclopramide (hypertension), voriconazole-budesonide for inhalation (increased serum concentration of budesonide), and levofloxacin-amiodarone (QT prolongation). The antimicrobial-drug pairs with a higher occurrence of actual DDIs included linezolid-dopamine/dobutamine (hypertension), fluconazole-amiodarone/ritonavir (QT prolongation), and cefoperazone/vancomycin-furosemide (nephrotoxicity). Moderate agreement existed between the two databases for pDDIs detection (Cohen's kappa = 0.546), but severity ratings diverged. Multivariable analysis identified the number of drugs per patient (OR = 1.178, p < 0.001), the number of antimicrobials per patient (OR = 1.146, p < 0.038), and the length of stay in the ICU (OR = 1.093, p < 0.038) as significant risk factors.</p><p><strong>Conclusions: </strong>High pDDI rates involving antimicrobials were observed in ICU patients, though actual DDIs were infrequent. Notable severe risk pairs warrant vigilant monitoring, especially with a higher occurrence of actual DDIs. Discrepancies in DDI databases emphasize the need for multi-tool validation to optimize medication safety.</p>\",\"PeriodicalId\":9023,\"journal\":{\"name\":\"BMC Pharmacology & Toxicology\",\"volume\":\"26 1\",\"pages\":\"104\"},\"PeriodicalIF\":2.7000,\"publicationDate\":\"2025-05-14\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12076841/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"BMC Pharmacology & Toxicology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1186/s40360-025-00925-z\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"PHARMACOLOGY & PHARMACY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMC Pharmacology & Toxicology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s40360-025-00925-z","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"PHARMACOLOGY & PHARMACY","Score":null,"Total":0}
Prevalence and clinical significance of potential drug-drug interactions of antimicrobials in Intensive Care Unit patients: a retrospective study.
Background: Antimicrobials are frequently prescribed in Intensive Care Units (ICUs), where drug-drug interactions (DDIs) with other medications may exacerbate clinical outcomes. Limited evidence exists on the prevalence and clinical impact of these interactions.
Objective: To estimate the prevalence of potential DDIs (pDDIs) between antimicrobials and other drugs in ICU patients using two electronic DDIs databases, identify the actual DDIs and the most frequently implicated antimicrobials, and determine the risk factors associated with actual DDIs.
Methods: We conducted a retrospective study on patients admitted to intensive care units from January to December 2023. Micromedex and Lexi-Interact were used to identify pDDIs and their severities. Furthermore, we used the Drug Interaction Probability Scale (DIPS) criteria to identify actual DDIs.
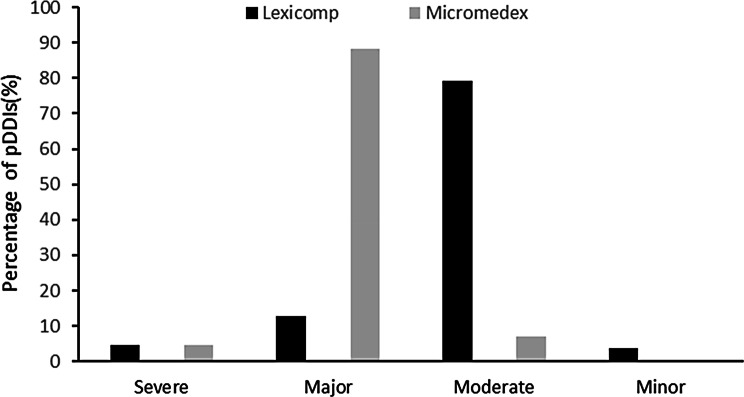
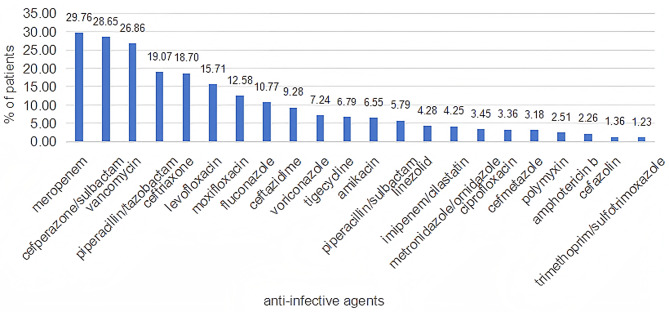
Results: Among 2,154 patients, 2,163 pDDIs (108 unique pairs) were identified in 461 patients, and 2.87% (62 pDDIs in 46 patients) were classified as actual DDIs. The antimicrobials most likely to cause pDDIs included quinolones, triazole antifungals, and linezolid. Antimicrobial-drug pairs with a higher incidence of severe pDDIs included linezolid-dopamine/metoclopramide (hypertension), voriconazole-budesonide for inhalation (increased serum concentration of budesonide), and levofloxacin-amiodarone (QT prolongation). The antimicrobial-drug pairs with a higher occurrence of actual DDIs included linezolid-dopamine/dobutamine (hypertension), fluconazole-amiodarone/ritonavir (QT prolongation), and cefoperazone/vancomycin-furosemide (nephrotoxicity). Moderate agreement existed between the two databases for pDDIs detection (Cohen's kappa = 0.546), but severity ratings diverged. Multivariable analysis identified the number of drugs per patient (OR = 1.178, p < 0.001), the number of antimicrobials per patient (OR = 1.146, p < 0.038), and the length of stay in the ICU (OR = 1.093, p < 0.038) as significant risk factors.
Conclusions: High pDDI rates involving antimicrobials were observed in ICU patients, though actual DDIs were infrequent. Notable severe risk pairs warrant vigilant monitoring, especially with a higher occurrence of actual DDIs. Discrepancies in DDI databases emphasize the need for multi-tool validation to optimize medication safety.
期刊介绍:
BMC Pharmacology and Toxicology is an open access, peer-reviewed journal that considers articles on all aspects of chemically defined therapeutic and toxic agents. The journal welcomes submissions from all fields of experimental and clinical pharmacology including clinical trials and toxicology.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


