Abdulrahim Y Mehadi, Bekure B Siraw, Parth Patel, Eli A Zaher, Ebrahim A Mohamed, Shahin Isha, Abel Tenaw Tasamma, Yordanos T Tafesse, Yonas Gebrecherkos, Juveriya Yasmeen, Mouaz Oudih, Mohammed Haroun
{"title":"房颤对内窥镜逆行胆管造影后住院结果的影响:2016-2020年全国住院患者样本的倾向评分匹配分析","authors":"Abdulrahim Y Mehadi, Bekure B Siraw, Parth Patel, Eli A Zaher, Ebrahim A Mohamed, Shahin Isha, Abel Tenaw Tasamma, Yordanos T Tafesse, Yonas Gebrecherkos, Juveriya Yasmeen, Mouaz Oudih, Mohammed Haroun","doi":"10.20524/aog.2025.0964","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Endoscopic retrograde cholangiopancreatography (ERCP) is a critical tool in managing hepatobiliary and pancreatic diseases. Atrial fibrillation (AF) has been associated with greater morbidity in patients undergoing ERCP. This study compared in-hospital ERCP outcomes in patients with and without AF.</p><p><strong>Methods: </strong>This retrospective cohort study utilized data from the National Inpatient Sample (2016-2020). Patients who underwent ERCP during hospitalization were included. Patients with AF were matched 1:1 to those without AF, based on demographic and clinical variables. The primary outcome was all-cause in-hospital mortality. Secondary outcomes included procedure-related and non-procedure-related complications, hospitalization cost and length of stay.</p><p><strong>Results: </strong>The final matched sample consisted of 29,942 patients, with 14,971 in each group (AF and non-AF). Patients with AF demonstrated significantly higher in-hospital mortality compared to those without AF (3.6% vs. 1.9%; odds ratio [OR] 1.87, 95% confidence interval [CI] 1.62-2.17). The AF group had a significantly longer median length of stay (8.1 vs. 6.4 days; β 1.7; 95%CI 1.5-1.8) and incurred higher hospitalization costs ($111,000 vs. $87,255; β $23,745; 95%CI $20,783-26,708). In terms of complications, patients with AF had significantly higher rates of acute kidney injury (OR 1.33, 95%CI 1.27-1.40) and sepsis (OR 1.38, 95%CI 1.30-1.48). However, the rates of procedure-specific complications, including biliary perforation, post-ERCP pancreatitis and post-ERCP cholangitis, were similar between the 2 groups.</p><p><strong>Conclusion: </strong>Patients with AF undergoing ERCP have higher in-hospital mortality, longer stays, greater costs, and higher rates of acute kidney injury and sepsis, although procedure-specific complication rates remain unaffected.</p>","PeriodicalId":7978,"journal":{"name":"Annals of Gastroenterology","volume":"38 3","pages":"345-352"},"PeriodicalIF":2.2000,"publicationDate":"2025-05-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12070335/pdf/","citationCount":"0","resultStr":"{\"title\":\"Impact of atrial fibrillation on in-hospital outcomes following endoscopic retrograde cholangiopancreatography: a propensity score-matched analysis of the National Inpatient Sample (2016-2020).\",\"authors\":\"Abdulrahim Y Mehadi, Bekure B Siraw, Parth Patel, Eli A Zaher, Ebrahim A Mohamed, Shahin Isha, Abel Tenaw Tasamma, Yordanos T Tafesse, Yonas Gebrecherkos, Juveriya Yasmeen, Mouaz Oudih, Mohammed Haroun\",\"doi\":\"10.20524/aog.2025.0964\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Endoscopic retrograde cholangiopancreatography (ERCP) is a critical tool in managing hepatobiliary and pancreatic diseases. Atrial fibrillation (AF) has been associated with greater morbidity in patients undergoing ERCP. This study compared in-hospital ERCP outcomes in patients with and without AF.</p><p><strong>Methods: </strong>This retrospective cohort study utilized data from the National Inpatient Sample (2016-2020). Patients who underwent ERCP during hospitalization were included. Patients with AF were matched 1:1 to those without AF, based on demographic and clinical variables. The primary outcome was all-cause in-hospital mortality. Secondary outcomes included procedure-related and non-procedure-related complications, hospitalization cost and length of stay.</p><p><strong>Results: </strong>The final matched sample consisted of 29,942 patients, with 14,971 in each group (AF and non-AF). Patients with AF demonstrated significantly higher in-hospital mortality compared to those without AF (3.6% vs. 1.9%; odds ratio [OR] 1.87, 95% confidence interval [CI] 1.62-2.17). The AF group had a significantly longer median length of stay (8.1 vs. 6.4 days; β 1.7; 95%CI 1.5-1.8) and incurred higher hospitalization costs ($111,000 vs. $87,255; β $23,745; 95%CI $20,783-26,708). In terms of complications, patients with AF had significantly higher rates of acute kidney injury (OR 1.33, 95%CI 1.27-1.40) and sepsis (OR 1.38, 95%CI 1.30-1.48). However, the rates of procedure-specific complications, including biliary perforation, post-ERCP pancreatitis and post-ERCP cholangitis, were similar between the 2 groups.</p><p><strong>Conclusion: </strong>Patients with AF undergoing ERCP have higher in-hospital mortality, longer stays, greater costs, and higher rates of acute kidney injury and sepsis, although procedure-specific complication rates remain unaffected.</p>\",\"PeriodicalId\":7978,\"journal\":{\"name\":\"Annals of Gastroenterology\",\"volume\":\"38 3\",\"pages\":\"345-352\"},\"PeriodicalIF\":2.2000,\"publicationDate\":\"2025-05-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12070335/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Annals of Gastroenterology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.20524/aog.2025.0964\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/4/25 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of Gastroenterology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.20524/aog.2025.0964","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/4/25 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
Impact of atrial fibrillation on in-hospital outcomes following endoscopic retrograde cholangiopancreatography: a propensity score-matched analysis of the National Inpatient Sample (2016-2020).
Background: Endoscopic retrograde cholangiopancreatography (ERCP) is a critical tool in managing hepatobiliary and pancreatic diseases. Atrial fibrillation (AF) has been associated with greater morbidity in patients undergoing ERCP. This study compared in-hospital ERCP outcomes in patients with and without AF.
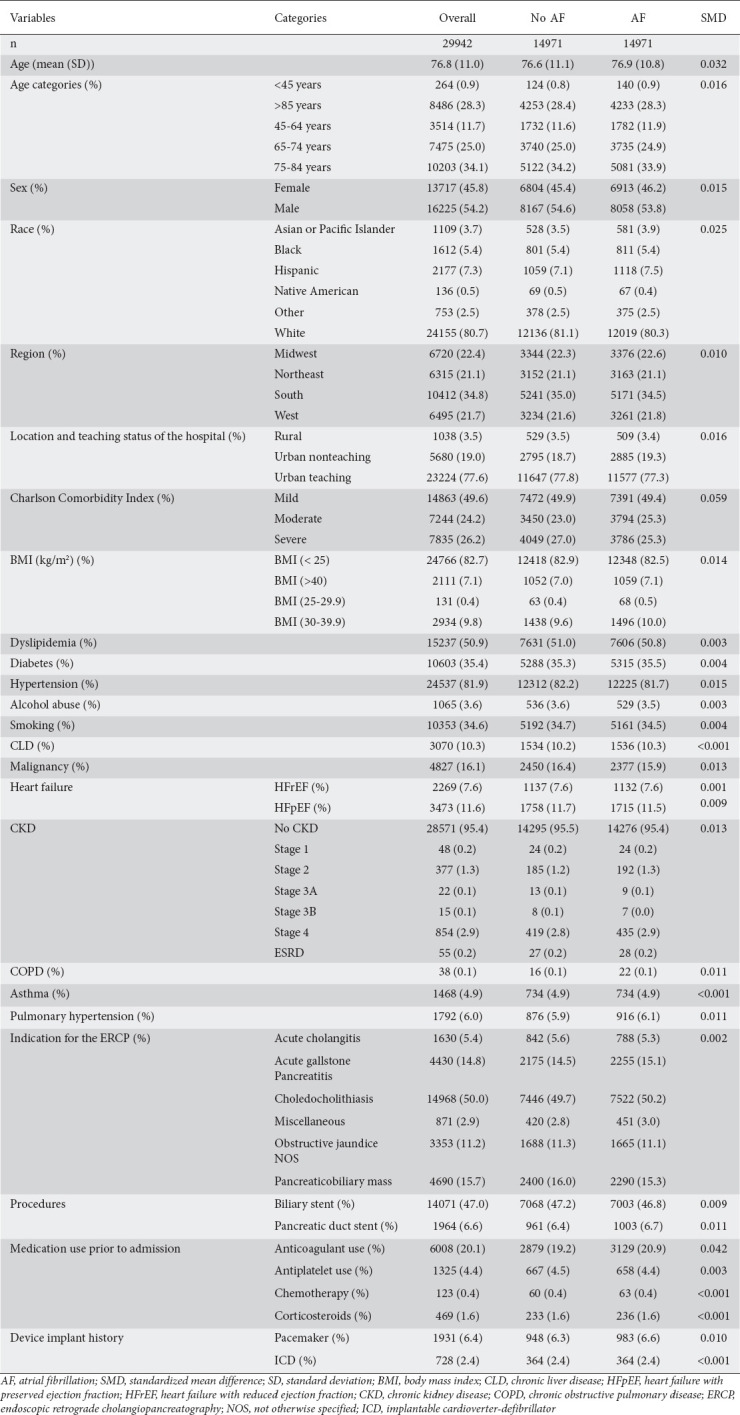
Methods: This retrospective cohort study utilized data from the National Inpatient Sample (2016-2020). Patients who underwent ERCP during hospitalization were included. Patients with AF were matched 1:1 to those without AF, based on demographic and clinical variables. The primary outcome was all-cause in-hospital mortality. Secondary outcomes included procedure-related and non-procedure-related complications, hospitalization cost and length of stay.
Results: The final matched sample consisted of 29,942 patients, with 14,971 in each group (AF and non-AF). Patients with AF demonstrated significantly higher in-hospital mortality compared to those without AF (3.6% vs. 1.9%; odds ratio [OR] 1.87, 95% confidence interval [CI] 1.62-2.17). The AF group had a significantly longer median length of stay (8.1 vs. 6.4 days; β 1.7; 95%CI 1.5-1.8) and incurred higher hospitalization costs ($111,000 vs. $87,255; β $23,745; 95%CI $20,783-26,708). In terms of complications, patients with AF had significantly higher rates of acute kidney injury (OR 1.33, 95%CI 1.27-1.40) and sepsis (OR 1.38, 95%CI 1.30-1.48). However, the rates of procedure-specific complications, including biliary perforation, post-ERCP pancreatitis and post-ERCP cholangitis, were similar between the 2 groups.
Conclusion: Patients with AF undergoing ERCP have higher in-hospital mortality, longer stays, greater costs, and higher rates of acute kidney injury and sepsis, although procedure-specific complication rates remain unaffected.



 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


