{"title":"高须动脉炎与多发性硬化的合并症:叙述回顾及病例报告。","authors":"Andrea Wesser, Andreas Albert Braun","doi":"10.1159/000545237","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Takayasu arteritis (TA) and multiple sclerosis (MS) are both immune-mediated diseases that can coexist, with TA causing vascular inflammation and MS involving demyelination driven by aberrant T-cell activity. The overlap of these conditions highlights shared immune mechanisms, such as T-cell dysregulation and cytokine release, underscoring the need for a nuanced understanding of their interplay, which is explored in a narrative review of reported cases.</p><p><strong>Case presentation: </strong>We narrate all reported cases of TA in patients with MS and report the case of a 57-year-old woman with MS with suspected bilateral optic neuritis and typical contrast-medium enhancement in both optic nerves. Because of normal visual acuity on both eyes, malignant hypertension, and fundoscopic findings indicative of hypertensive retinopathy, we diagnosed hypertensive retinopathy with secondary contrast-medium enhancement of the optic nerves. We established antihypertensive medication and searched for secondary causes of hypertension and highly elevated erythrocyte sedimentation rate, which led to the finding of large vessel wall inflammation and the diagnosis of TA.</p><p><strong>Conclusion: </strong>TA can present with a variety of ocular symptoms, including hypertensive retinopathy, retinal ischemia, and anterior ischemic optic neuropathy, often mimicking other diseases. While rare, the coexistence of TA and MS, including cases associated with interferon-beta therapy, suggests shared immune mechanisms and underscores the need for careful monitoring of patients with MS receiving immunomodulatory treatments. The broad spectrum of potential causes for optic nerve abnormalities necessitates a thorough evaluation to avoid misdiagnosis and ensure appropriate treatment.</p>","PeriodicalId":101351,"journal":{"name":"Biomedicine hub","volume":"10 1","pages":"72-80"},"PeriodicalIF":0.0000,"publicationDate":"2025-03-20","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12028982/pdf/","citationCount":"0","resultStr":"{\"title\":\"Coincidence of Takayasu Arteritis and Multiple Sclerosis: Narrative Review and Case Report.\",\"authors\":\"Andrea Wesser, Andreas Albert Braun\",\"doi\":\"10.1159/000545237\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Takayasu arteritis (TA) and multiple sclerosis (MS) are both immune-mediated diseases that can coexist, with TA causing vascular inflammation and MS involving demyelination driven by aberrant T-cell activity. The overlap of these conditions highlights shared immune mechanisms, such as T-cell dysregulation and cytokine release, underscoring the need for a nuanced understanding of their interplay, which is explored in a narrative review of reported cases.</p><p><strong>Case presentation: </strong>We narrate all reported cases of TA in patients with MS and report the case of a 57-year-old woman with MS with suspected bilateral optic neuritis and typical contrast-medium enhancement in both optic nerves. Because of normal visual acuity on both eyes, malignant hypertension, and fundoscopic findings indicative of hypertensive retinopathy, we diagnosed hypertensive retinopathy with secondary contrast-medium enhancement of the optic nerves. We established antihypertensive medication and searched for secondary causes of hypertension and highly elevated erythrocyte sedimentation rate, which led to the finding of large vessel wall inflammation and the diagnosis of TA.</p><p><strong>Conclusion: </strong>TA can present with a variety of ocular symptoms, including hypertensive retinopathy, retinal ischemia, and anterior ischemic optic neuropathy, often mimicking other diseases. While rare, the coexistence of TA and MS, including cases associated with interferon-beta therapy, suggests shared immune mechanisms and underscores the need for careful monitoring of patients with MS receiving immunomodulatory treatments. The broad spectrum of potential causes for optic nerve abnormalities necessitates a thorough evaluation to avoid misdiagnosis and ensure appropriate treatment.</p>\",\"PeriodicalId\":101351,\"journal\":{\"name\":\"Biomedicine hub\",\"volume\":\"10 1\",\"pages\":\"72-80\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2025-03-20\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12028982/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Biomedicine hub\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1159/000545237\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Biomedicine hub","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1159/000545237","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
Coincidence of Takayasu Arteritis and Multiple Sclerosis: Narrative Review and Case Report.
Introduction: Takayasu arteritis (TA) and multiple sclerosis (MS) are both immune-mediated diseases that can coexist, with TA causing vascular inflammation and MS involving demyelination driven by aberrant T-cell activity. The overlap of these conditions highlights shared immune mechanisms, such as T-cell dysregulation and cytokine release, underscoring the need for a nuanced understanding of their interplay, which is explored in a narrative review of reported cases.
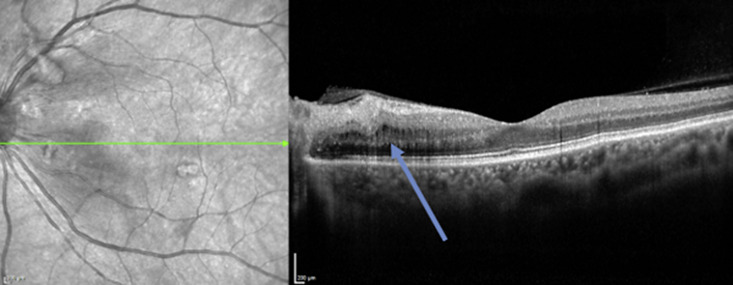
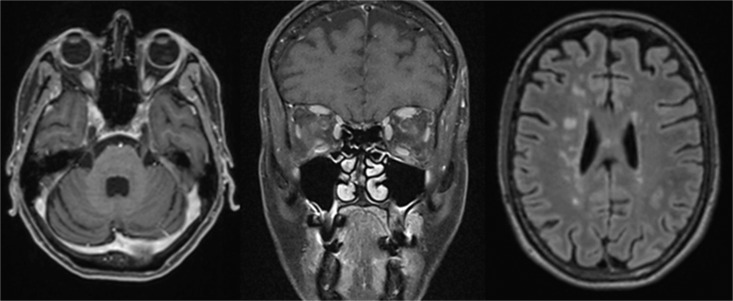
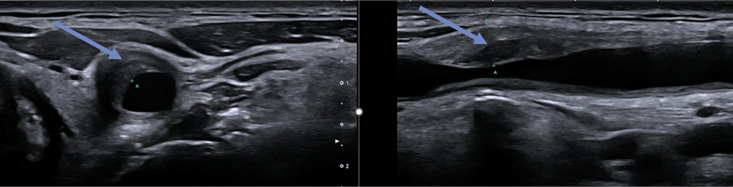
Case presentation: We narrate all reported cases of TA in patients with MS and report the case of a 57-year-old woman with MS with suspected bilateral optic neuritis and typical contrast-medium enhancement in both optic nerves. Because of normal visual acuity on both eyes, malignant hypertension, and fundoscopic findings indicative of hypertensive retinopathy, we diagnosed hypertensive retinopathy with secondary contrast-medium enhancement of the optic nerves. We established antihypertensive medication and searched for secondary causes of hypertension and highly elevated erythrocyte sedimentation rate, which led to the finding of large vessel wall inflammation and the diagnosis of TA.
Conclusion: TA can present with a variety of ocular symptoms, including hypertensive retinopathy, retinal ischemia, and anterior ischemic optic neuropathy, often mimicking other diseases. While rare, the coexistence of TA and MS, including cases associated with interferon-beta therapy, suggests shared immune mechanisms and underscores the need for careful monitoring of patients with MS receiving immunomodulatory treatments. The broad spectrum of potential causes for optic nerve abnormalities necessitates a thorough evaluation to avoid misdiagnosis and ensure appropriate treatment.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


