Zhe Zhang, Shanshan Jin, Bin Liu, Hai Feng, Wenrui Li
{"title":"急性肺栓塞患者导管溶栓与机械抽吸的临床效果。","authors":"Zhe Zhang, Shanshan Jin, Bin Liu, Hai Feng, Wenrui Li","doi":"10.5761/atcs.oa.25-00012","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>The objective of this study was to evaluate the safety and efficacy of catheter-directed thrombolysis (CDT) and mechanical aspiration (MA) for acute pulmonary embolism (PE).</p><p><strong>Methods: </strong>From February 2022 to October 2024, the clinical data of patients with high- and intermediate-risk PE who received endovascular therapy were retrospectively reviewed. Patients were categorized based on the treatment strategy.</p><p><strong>Results: </strong>Fifty-eight consecutive patients were identified. CDT was initiated in 29 patients, while the remaining 29 received MA treatment. The time of thrombolysis and the dosage of urokinase were both lower in the MA group (P <0.05). No differences were found in cardiac biomarkers after 48 hours, perioperative bleeding events, heart/valve injury, and mortality. The total cost of the MA group was much higher compared to CDT alone. The MA group showed better improvement in right ventricular (RV) function with a higher reduction in the right ventricular-to-left ventricular ratio (0.55 ± 0.46 vs. 0.13 ± 0.53, P = 0.017). No differences were found in the reduction of the CT obstruction index.</p><p><strong>Conclusion: </strong>CDT and MA seem to have similar outcomes for patients with acute high- and intermediate-risk PE. MA is more effective in improving RV function with less thrombolysis time and fewer thrombolytics.</p>","PeriodicalId":93877,"journal":{"name":"Annals of thoracic and cardiovascular surgery : official journal of the Association of Thoracic and Cardiovascular Surgeons of Asia","volume":"31 1","pages":""},"PeriodicalIF":1.3000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12009743/pdf/","citationCount":"0","resultStr":"{\"title\":\"Clinical Outcomes of Catheter-Directed Thrombolysis versus Mechanical Aspiration in Patients with Acute Pulmonary Embolism.\",\"authors\":\"Zhe Zhang, Shanshan Jin, Bin Liu, Hai Feng, Wenrui Li\",\"doi\":\"10.5761/atcs.oa.25-00012\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Purpose: </strong>The objective of this study was to evaluate the safety and efficacy of catheter-directed thrombolysis (CDT) and mechanical aspiration (MA) for acute pulmonary embolism (PE).</p><p><strong>Methods: </strong>From February 2022 to October 2024, the clinical data of patients with high- and intermediate-risk PE who received endovascular therapy were retrospectively reviewed. Patients were categorized based on the treatment strategy.</p><p><strong>Results: </strong>Fifty-eight consecutive patients were identified. CDT was initiated in 29 patients, while the remaining 29 received MA treatment. The time of thrombolysis and the dosage of urokinase were both lower in the MA group (P <0.05). No differences were found in cardiac biomarkers after 48 hours, perioperative bleeding events, heart/valve injury, and mortality. The total cost of the MA group was much higher compared to CDT alone. The MA group showed better improvement in right ventricular (RV) function with a higher reduction in the right ventricular-to-left ventricular ratio (0.55 ± 0.46 vs. 0.13 ± 0.53, P = 0.017). No differences were found in the reduction of the CT obstruction index.</p><p><strong>Conclusion: </strong>CDT and MA seem to have similar outcomes for patients with acute high- and intermediate-risk PE. MA is more effective in improving RV function with less thrombolysis time and fewer thrombolytics.</p>\",\"PeriodicalId\":93877,\"journal\":{\"name\":\"Annals of thoracic and cardiovascular surgery : official journal of the Association of Thoracic and Cardiovascular Surgeons of Asia\",\"volume\":\"31 1\",\"pages\":\"\"},\"PeriodicalIF\":1.3000,\"publicationDate\":\"2025-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12009743/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Annals of thoracic and cardiovascular surgery : official journal of the Association of Thoracic and Cardiovascular Surgeons of Asia\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.5761/atcs.oa.25-00012\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of thoracic and cardiovascular surgery : official journal of the Association of Thoracic and Cardiovascular Surgeons of Asia","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5761/atcs.oa.25-00012","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Clinical Outcomes of Catheter-Directed Thrombolysis versus Mechanical Aspiration in Patients with Acute Pulmonary Embolism.
Purpose: The objective of this study was to evaluate the safety and efficacy of catheter-directed thrombolysis (CDT) and mechanical aspiration (MA) for acute pulmonary embolism (PE).
Methods: From February 2022 to October 2024, the clinical data of patients with high- and intermediate-risk PE who received endovascular therapy were retrospectively reviewed. Patients were categorized based on the treatment strategy.
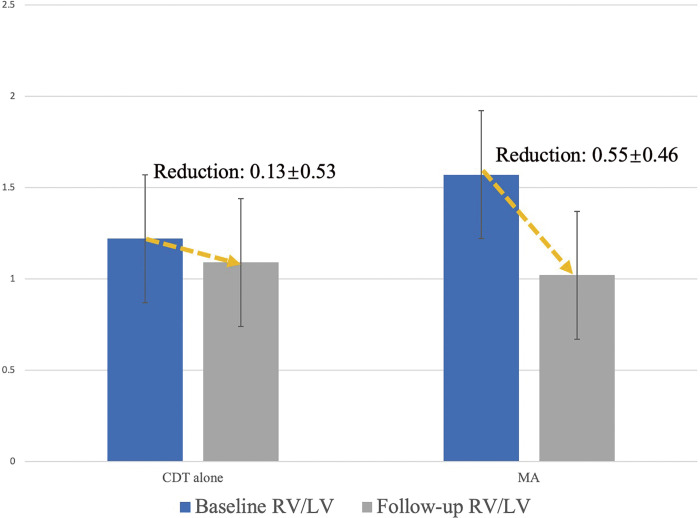
Results: Fifty-eight consecutive patients were identified. CDT was initiated in 29 patients, while the remaining 29 received MA treatment. The time of thrombolysis and the dosage of urokinase were both lower in the MA group (P <0.05). No differences were found in cardiac biomarkers after 48 hours, perioperative bleeding events, heart/valve injury, and mortality. The total cost of the MA group was much higher compared to CDT alone. The MA group showed better improvement in right ventricular (RV) function with a higher reduction in the right ventricular-to-left ventricular ratio (0.55 ± 0.46 vs. 0.13 ± 0.53, P = 0.017). No differences were found in the reduction of the CT obstruction index.
Conclusion: CDT and MA seem to have similar outcomes for patients with acute high- and intermediate-risk PE. MA is more effective in improving RV function with less thrombolysis time and fewer thrombolytics.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


