{"title":"双侧机器人全膝关节置换术中机械对齐和功能对齐的比较效果:一项随机对照试验。","authors":"Thakrit Chompoosang, Utain Ketkaewsuwan, Patcharavit Ploynumpon","doi":"10.1186/s42836-025-00310-5","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Functional alignment (FA) in total knee arthroplasty (TKA) can achieve soft tissue balance by fine-tuning adjustments of bony resections and component alignment with less soft tissue release. However, joint line orientation relative to the floor in the knee and ankle after TKA is not well studied.</p><p><strong>Methods: </strong>A randomized-controlled trial was performed in 30 patients with robotic-assisted bilateral TKA using FA and mechanical alignment (MA) in the same patient. The outcome measures were as follows: (1) standing radiographic knee and ankle alignment; (2) clinical outcomes at 1, 3 and 6 months postoperatively (including forgotten joint score (FJS), KOOS, knee range of motion); (3) patient satisfaction score; and (4) soft tissue release.</p><p><strong>Results: </strong>Postoperative hip-knee-ankle angles between the FA and MA groups were similar (2.4° versus 2.4°, P = 0.952). Knee joint line orientation was significantly more parallel to the floor in the FA group (3.0° versus 4.7°, P < 0.001). There was no significant difference in ankle joint line orientation relative to the floor in the FA and MA groups (91.0° versus 92.4°, P = 0.099 for tibial plafond inclination and 92.5° versus 93.2°, P = 0.564 for talar dome inclination). However, in knees with preoperative varus with apex distal joint line orientation (coronal plane alignment of the knee (CPAK) classification type I), FA significantly achieved a more parallel knee and ankle joint line orientation relative to the floor (3.1° versus 5.1°, P = 0.002 for knee and 91.0° versus 93.5°, P = 0.028 for tibial plafond inclination). FA can obtain a balanced knee with significantly lower posteromedial releases (23.3% versus 76.7%, P < 0.001), with no superficial MCL release needed (0% versus 6.67%, P < 0.01). The FA group achieved significantly higher FJS at 3 months (53.3 versus 46.0, P = 0.015) and 6 months (67.8 versus 57.8, P < 0.001) with a higher patient satisfaction score (79.2 versus 84.3, P = 0.001).</p><p><strong>Conclusion: </strong>Functional alignment can control the overall lower limb alignment similarly to mechanical alignment, with a knee joint line more parallel to the floor. Additionally, the ankle joint line was more parallel in knees with CPAK type I. FA can also provide a more balanced knee with less soft tissue release, a higher functional score, and greater patient satisfaction compared to mechanical alignment.</p>","PeriodicalId":52831,"journal":{"name":"Arthroplasty","volume":"7 1","pages":"25"},"PeriodicalIF":4.3000,"publicationDate":"2025-05-07","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12057096/pdf/","citationCount":"0","resultStr":"{\"title\":\"Comparative effects of mechanical and functional alignment in bilateral robotic total knee arthroplasty: a randomized controlled trial.\",\"authors\":\"Thakrit Chompoosang, Utain Ketkaewsuwan, Patcharavit Ploynumpon\",\"doi\":\"10.1186/s42836-025-00310-5\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Functional alignment (FA) in total knee arthroplasty (TKA) can achieve soft tissue balance by fine-tuning adjustments of bony resections and component alignment with less soft tissue release. However, joint line orientation relative to the floor in the knee and ankle after TKA is not well studied.</p><p><strong>Methods: </strong>A randomized-controlled trial was performed in 30 patients with robotic-assisted bilateral TKA using FA and mechanical alignment (MA) in the same patient. The outcome measures were as follows: (1) standing radiographic knee and ankle alignment; (2) clinical outcomes at 1, 3 and 6 months postoperatively (including forgotten joint score (FJS), KOOS, knee range of motion); (3) patient satisfaction score; and (4) soft tissue release.</p><p><strong>Results: </strong>Postoperative hip-knee-ankle angles between the FA and MA groups were similar (2.4° versus 2.4°, P = 0.952). Knee joint line orientation was significantly more parallel to the floor in the FA group (3.0° versus 4.7°, P < 0.001). There was no significant difference in ankle joint line orientation relative to the floor in the FA and MA groups (91.0° versus 92.4°, P = 0.099 for tibial plafond inclination and 92.5° versus 93.2°, P = 0.564 for talar dome inclination). However, in knees with preoperative varus with apex distal joint line orientation (coronal plane alignment of the knee (CPAK) classification type I), FA significantly achieved a more parallel knee and ankle joint line orientation relative to the floor (3.1° versus 5.1°, P = 0.002 for knee and 91.0° versus 93.5°, P = 0.028 for tibial plafond inclination). FA can obtain a balanced knee with significantly lower posteromedial releases (23.3% versus 76.7%, P < 0.001), with no superficial MCL release needed (0% versus 6.67%, P < 0.01). The FA group achieved significantly higher FJS at 3 months (53.3 versus 46.0, P = 0.015) and 6 months (67.8 versus 57.8, P < 0.001) with a higher patient satisfaction score (79.2 versus 84.3, P = 0.001).</p><p><strong>Conclusion: </strong>Functional alignment can control the overall lower limb alignment similarly to mechanical alignment, with a knee joint line more parallel to the floor. Additionally, the ankle joint line was more parallel in knees with CPAK type I. FA can also provide a more balanced knee with less soft tissue release, a higher functional score, and greater patient satisfaction compared to mechanical alignment.</p>\",\"PeriodicalId\":52831,\"journal\":{\"name\":\"Arthroplasty\",\"volume\":\"7 1\",\"pages\":\"25\"},\"PeriodicalIF\":4.3000,\"publicationDate\":\"2025-05-07\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12057096/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Arthroplasty\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1186/s42836-025-00310-5\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"ORTHOPEDICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Arthroplasty","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s42836-025-00310-5","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
Comparative effects of mechanical and functional alignment in bilateral robotic total knee arthroplasty: a randomized controlled trial.
Background: Functional alignment (FA) in total knee arthroplasty (TKA) can achieve soft tissue balance by fine-tuning adjustments of bony resections and component alignment with less soft tissue release. However, joint line orientation relative to the floor in the knee and ankle after TKA is not well studied.
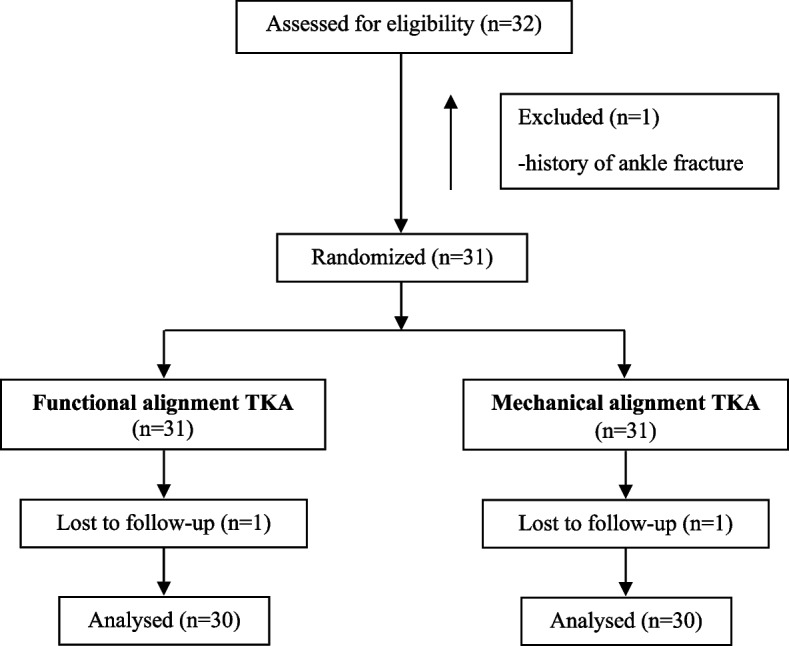
Methods: A randomized-controlled trial was performed in 30 patients with robotic-assisted bilateral TKA using FA and mechanical alignment (MA) in the same patient. The outcome measures were as follows: (1) standing radiographic knee and ankle alignment; (2) clinical outcomes at 1, 3 and 6 months postoperatively (including forgotten joint score (FJS), KOOS, knee range of motion); (3) patient satisfaction score; and (4) soft tissue release.
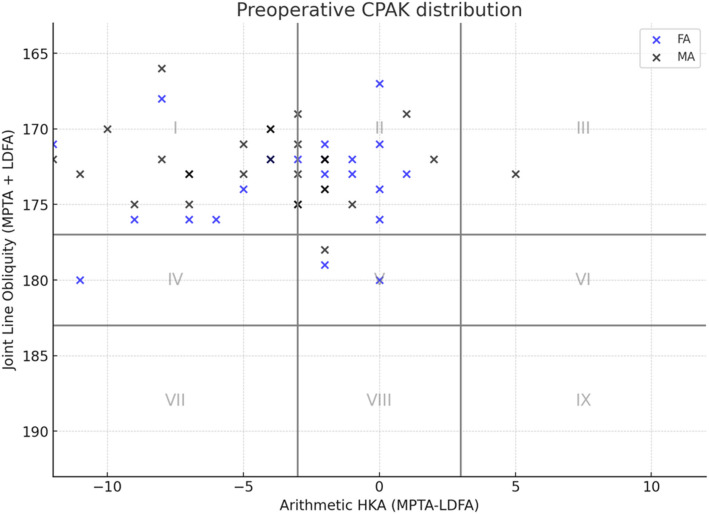
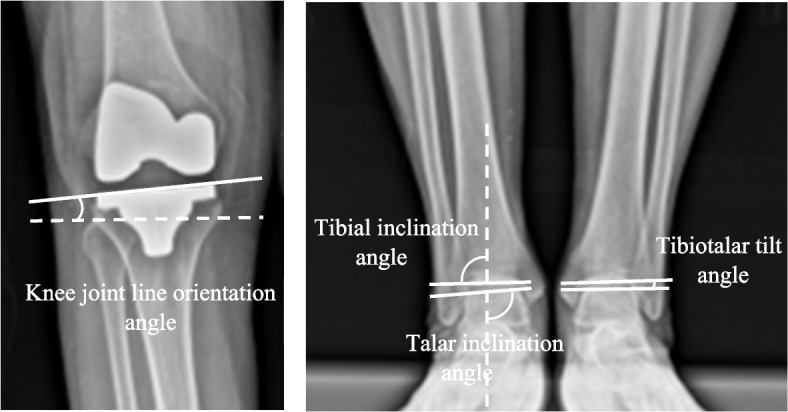
Results: Postoperative hip-knee-ankle angles between the FA and MA groups were similar (2.4° versus 2.4°, P = 0.952). Knee joint line orientation was significantly more parallel to the floor in the FA group (3.0° versus 4.7°, P < 0.001). There was no significant difference in ankle joint line orientation relative to the floor in the FA and MA groups (91.0° versus 92.4°, P = 0.099 for tibial plafond inclination and 92.5° versus 93.2°, P = 0.564 for talar dome inclination). However, in knees with preoperative varus with apex distal joint line orientation (coronal plane alignment of the knee (CPAK) classification type I), FA significantly achieved a more parallel knee and ankle joint line orientation relative to the floor (3.1° versus 5.1°, P = 0.002 for knee and 91.0° versus 93.5°, P = 0.028 for tibial plafond inclination). FA can obtain a balanced knee with significantly lower posteromedial releases (23.3% versus 76.7%, P < 0.001), with no superficial MCL release needed (0% versus 6.67%, P < 0.01). The FA group achieved significantly higher FJS at 3 months (53.3 versus 46.0, P = 0.015) and 6 months (67.8 versus 57.8, P < 0.001) with a higher patient satisfaction score (79.2 versus 84.3, P = 0.001).
Conclusion: Functional alignment can control the overall lower limb alignment similarly to mechanical alignment, with a knee joint line more parallel to the floor. Additionally, the ankle joint line was more parallel in knees with CPAK type I. FA can also provide a more balanced knee with less soft tissue release, a higher functional score, and greater patient satisfaction compared to mechanical alignment.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


