John A Henry, Susannah M Black, Oliver G J Mitchell, Edward Richardson, Cameron Watson, Chris Hare, Pierre Le Page, Andrew R J Mitchell
{"title":"心血管计算机断层扫描的冠状动脉炎症和人工智能风险评分:对现实世界中风险预测和临床管理的影响","authors":"John A Henry, Susannah M Black, Oliver G J Mitchell, Edward Richardson, Cameron Watson, Chris Hare, Pierre Le Page, Andrew R J Mitchell","doi":"10.1093/ehjimp/qyaf031","DOIUrl":null,"url":null,"abstract":"<p><strong>Aims: </strong>Coronary computed tomography angiography (CCTA) is the primary investigation for stable chest pain. Despite approximately 80% of individuals undergoing CCTA not having obstructive coronary disease, this group contributes to two-thirds of major adverse cardiovascular events. Assessment of coronary inflammation using perivascular fat attenuation index (FAI) and AI-derived risk scores (AI-Risk) has demonstrated enhanced risk prediction beyond traditional clinical and CCTA parameters. We aimed to assess if FAI and AI-Risk alter risk prediction and clinical management in a real-world setting.</p><p><strong>Methods and results: </strong>Consecutive patients undergoing CCTA with FAI calculation and AI-Risk (CaRi-Heart®) at a single centre over a 3-year period were recruited. Conventional risk scores for non-fatal and fatal myocardial infarctions (QRISK3 and SCORE, respectively) were compared with AI-Risk. Clinical management decisions based on risk factors and CCTA results were recorded. FAI and AI-Risk scores were then provided and the resultant clinical management decision recorded. One hundred and sixty-four patients were included in the study (<i>n</i> = 164, male 78%, 56 years). Forty-eight per cent of the patients had no evidence of coronary artery disease (CAD) on CCTA, with 41% having non-obstructive CAD and 10% with potentially obstructive CAD. AI-Risk reclassified risk in 58% and 43% of patients compared with QRISK3 and SCORE, respectively. Clinical management was changed in 33% of patients following AI-Risk analysis.</p><p><strong>Conclusion: </strong>FAI and AI-Risk scores in a real-world setting changed risk prediction in around half of individuals and changed clinical management in around a third.</p>","PeriodicalId":94317,"journal":{"name":"European heart journal. Imaging methods and practice","volume":"2 4","pages":"qyaf031"},"PeriodicalIF":0.0000,"publicationDate":"2025-04-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12003852/pdf/","citationCount":"0","resultStr":"{\"title\":\"Coronary inflammation and AI-Risk scores from cardiovascular computed tomography: impact on risk prediction and clinical management in a real-world setting.\",\"authors\":\"John A Henry, Susannah M Black, Oliver G J Mitchell, Edward Richardson, Cameron Watson, Chris Hare, Pierre Le Page, Andrew R J Mitchell\",\"doi\":\"10.1093/ehjimp/qyaf031\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Aims: </strong>Coronary computed tomography angiography (CCTA) is the primary investigation for stable chest pain. Despite approximately 80% of individuals undergoing CCTA not having obstructive coronary disease, this group contributes to two-thirds of major adverse cardiovascular events. Assessment of coronary inflammation using perivascular fat attenuation index (FAI) and AI-derived risk scores (AI-Risk) has demonstrated enhanced risk prediction beyond traditional clinical and CCTA parameters. We aimed to assess if FAI and AI-Risk alter risk prediction and clinical management in a real-world setting.</p><p><strong>Methods and results: </strong>Consecutive patients undergoing CCTA with FAI calculation and AI-Risk (CaRi-Heart®) at a single centre over a 3-year period were recruited. Conventional risk scores for non-fatal and fatal myocardial infarctions (QRISK3 and SCORE, respectively) were compared with AI-Risk. Clinical management decisions based on risk factors and CCTA results were recorded. FAI and AI-Risk scores were then provided and the resultant clinical management decision recorded. One hundred and sixty-four patients were included in the study (<i>n</i> = 164, male 78%, 56 years). Forty-eight per cent of the patients had no evidence of coronary artery disease (CAD) on CCTA, with 41% having non-obstructive CAD and 10% with potentially obstructive CAD. AI-Risk reclassified risk in 58% and 43% of patients compared with QRISK3 and SCORE, respectively. Clinical management was changed in 33% of patients following AI-Risk analysis.</p><p><strong>Conclusion: </strong>FAI and AI-Risk scores in a real-world setting changed risk prediction in around half of individuals and changed clinical management in around a third.</p>\",\"PeriodicalId\":94317,\"journal\":{\"name\":\"European heart journal. Imaging methods and practice\",\"volume\":\"2 4\",\"pages\":\"qyaf031\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2025-04-17\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12003852/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"European heart journal. Imaging methods and practice\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1093/ehjimp/qyaf031\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/10/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"European heart journal. Imaging methods and practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/ehjimp/qyaf031","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/10/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
Coronary inflammation and AI-Risk scores from cardiovascular computed tomography: impact on risk prediction and clinical management in a real-world setting.
Aims: Coronary computed tomography angiography (CCTA) is the primary investigation for stable chest pain. Despite approximately 80% of individuals undergoing CCTA not having obstructive coronary disease, this group contributes to two-thirds of major adverse cardiovascular events. Assessment of coronary inflammation using perivascular fat attenuation index (FAI) and AI-derived risk scores (AI-Risk) has demonstrated enhanced risk prediction beyond traditional clinical and CCTA parameters. We aimed to assess if FAI and AI-Risk alter risk prediction and clinical management in a real-world setting.
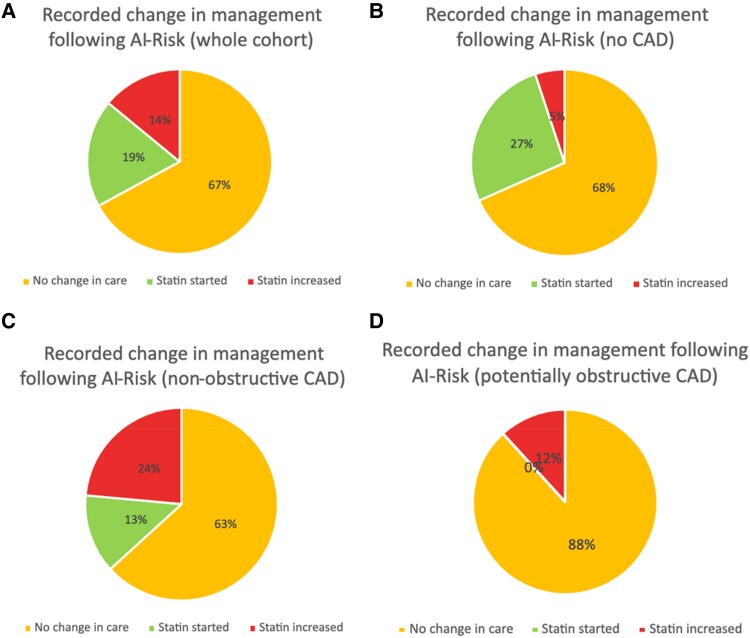
Methods and results: Consecutive patients undergoing CCTA with FAI calculation and AI-Risk (CaRi-Heart®) at a single centre over a 3-year period were recruited. Conventional risk scores for non-fatal and fatal myocardial infarctions (QRISK3 and SCORE, respectively) were compared with AI-Risk. Clinical management decisions based on risk factors and CCTA results were recorded. FAI and AI-Risk scores were then provided and the resultant clinical management decision recorded. One hundred and sixty-four patients were included in the study (n = 164, male 78%, 56 years). Forty-eight per cent of the patients had no evidence of coronary artery disease (CAD) on CCTA, with 41% having non-obstructive CAD and 10% with potentially obstructive CAD. AI-Risk reclassified risk in 58% and 43% of patients compared with QRISK3 and SCORE, respectively. Clinical management was changed in 33% of patients following AI-Risk analysis.
Conclusion: FAI and AI-Risk scores in a real-world setting changed risk prediction in around half of individuals and changed clinical management in around a third.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


