{"title":"精氨酸刺激copeptin切断诊断AVP缺乏症(中枢性尿囊症)的事后内部验证。","authors":"Cihan Atila, Bettina Winzeler, Irina Chifu, Martin Fassnacht, Julie Refardt, Mirjam Christ-Crain","doi":"10.1007/s11102-025-01523-2","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Distinguishing arginine vasopressin (AVP) deficiency (central diabetes insipidus) from primary polydipsia is challenging. While hypertonic saline-stimulated copeptin testing provides the highest diagnostic accuracy, it is often restricted to specialised centres, requiring close monitoring and potentially causing patient discomfort. Initially, arginine-stimulated copeptin was proposed as a simpler alternative, but a head-to-head comparison study found it less precise than hypertonic saline stimulation. However, the same study identified two new high sensitivity and specificity cut-offs for arginine-stimulated copeptin, though these cut-offs have yet to be validated.</p><p><strong>Methods: </strong>This is a secondary post-hoc analysis of the initial prospective multicentre study, including adult patients with confirmed AVP deficiency or primary polydipsia. Participants underwent the arginine stimulation test, with plasma copeptin measured at baseline and 60- and 90 min after arginine infusion. The primary objective was to revisit the original study to internally validate the proposed arginine-stimulated copeptin cut-offs of > 5.2pmol/L (high specificity cut-off with > 90% specificity for primary polydipsia) and ≤ 3.0 pmol/L (high specificity cut-off with > 90% specificity for AVP deficiency).</p><p><strong>Findings: </strong>In total, 96 patients were included between May 2013 and June 2018: n = 38 [40%] with AVP deficiency and n = 58 [60%] with primary polydipsia. At 60 min after arginine infusion, a copeptin level ≤ 3.0 pmol/L showed a specificity of 95% (95% CI: 0.88-1.00) for AVP deficiency, while a copeptin level > 5.2 pmol/L demonstrated a specificity of 97% (95% CI: 0.92-1.00) for primary polydipsia. The ≤ 3.0 pmol/L cut-off accurately identified 71% (n = 27/38) of patients with AVP deficiency, and the > 5.2 pmol/L cut-off correctly identified 69% (n = 40/58) of patients with primary polydipsia.</p><p><strong>Interpretation: </strong>This analysis validates two new copeptin cut-offs of the arginine stimulation test to distinguish AVP deficiency from primary polydipsia: >5.2 pmol/L for high specificity in diagnosing primary polydipsia and ≤ 3.0 pmol/L for high specificity in diagnosing AVP deficiency. These thresholds might offer a practical initial alternative to hypertonic saline testing.</p><p><strong>Registration: </strong>Clinicaltrials.gov (NCT00757276).</p>","PeriodicalId":20202,"journal":{"name":"Pituitary","volume":"28 3","pages":"53"},"PeriodicalIF":3.4000,"publicationDate":"2025-04-26","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12031852/pdf/","citationCount":"0","resultStr":"{\"title\":\"A post-hoc internal validation of arginine-stimulated copeptin cut-offs for diagnosing AVP deficiency (central diabetes insipidus).\",\"authors\":\"Cihan Atila, Bettina Winzeler, Irina Chifu, Martin Fassnacht, Julie Refardt, Mirjam Christ-Crain\",\"doi\":\"10.1007/s11102-025-01523-2\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Distinguishing arginine vasopressin (AVP) deficiency (central diabetes insipidus) from primary polydipsia is challenging. While hypertonic saline-stimulated copeptin testing provides the highest diagnostic accuracy, it is often restricted to specialised centres, requiring close monitoring and potentially causing patient discomfort. Initially, arginine-stimulated copeptin was proposed as a simpler alternative, but a head-to-head comparison study found it less precise than hypertonic saline stimulation. However, the same study identified two new high sensitivity and specificity cut-offs for arginine-stimulated copeptin, though these cut-offs have yet to be validated.</p><p><strong>Methods: </strong>This is a secondary post-hoc analysis of the initial prospective multicentre study, including adult patients with confirmed AVP deficiency or primary polydipsia. Participants underwent the arginine stimulation test, with plasma copeptin measured at baseline and 60- and 90 min after arginine infusion. The primary objective was to revisit the original study to internally validate the proposed arginine-stimulated copeptin cut-offs of > 5.2pmol/L (high specificity cut-off with > 90% specificity for primary polydipsia) and ≤ 3.0 pmol/L (high specificity cut-off with > 90% specificity for AVP deficiency).</p><p><strong>Findings: </strong>In total, 96 patients were included between May 2013 and June 2018: n = 38 [40%] with AVP deficiency and n = 58 [60%] with primary polydipsia. At 60 min after arginine infusion, a copeptin level ≤ 3.0 pmol/L showed a specificity of 95% (95% CI: 0.88-1.00) for AVP deficiency, while a copeptin level > 5.2 pmol/L demonstrated a specificity of 97% (95% CI: 0.92-1.00) for primary polydipsia. The ≤ 3.0 pmol/L cut-off accurately identified 71% (n = 27/38) of patients with AVP deficiency, and the > 5.2 pmol/L cut-off correctly identified 69% (n = 40/58) of patients with primary polydipsia.</p><p><strong>Interpretation: </strong>This analysis validates two new copeptin cut-offs of the arginine stimulation test to distinguish AVP deficiency from primary polydipsia: >5.2 pmol/L for high specificity in diagnosing primary polydipsia and ≤ 3.0 pmol/L for high specificity in diagnosing AVP deficiency. These thresholds might offer a practical initial alternative to hypertonic saline testing.</p><p><strong>Registration: </strong>Clinicaltrials.gov (NCT00757276).</p>\",\"PeriodicalId\":20202,\"journal\":{\"name\":\"Pituitary\",\"volume\":\"28 3\",\"pages\":\"53\"},\"PeriodicalIF\":3.4000,\"publicationDate\":\"2025-04-26\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12031852/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Pituitary\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s11102-025-01523-2\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"ENDOCRINOLOGY & METABOLISM\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pituitary","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s11102-025-01523-2","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
A post-hoc internal validation of arginine-stimulated copeptin cut-offs for diagnosing AVP deficiency (central diabetes insipidus).
Background: Distinguishing arginine vasopressin (AVP) deficiency (central diabetes insipidus) from primary polydipsia is challenging. While hypertonic saline-stimulated copeptin testing provides the highest diagnostic accuracy, it is often restricted to specialised centres, requiring close monitoring and potentially causing patient discomfort. Initially, arginine-stimulated copeptin was proposed as a simpler alternative, but a head-to-head comparison study found it less precise than hypertonic saline stimulation. However, the same study identified two new high sensitivity and specificity cut-offs for arginine-stimulated copeptin, though these cut-offs have yet to be validated.
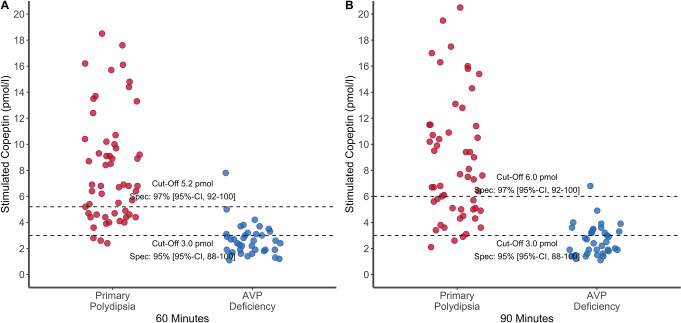
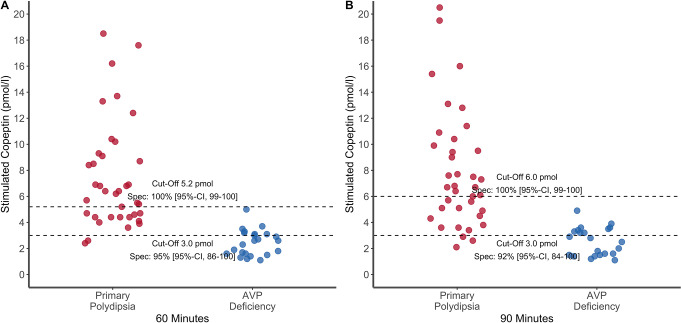
Methods: This is a secondary post-hoc analysis of the initial prospective multicentre study, including adult patients with confirmed AVP deficiency or primary polydipsia. Participants underwent the arginine stimulation test, with plasma copeptin measured at baseline and 60- and 90 min after arginine infusion. The primary objective was to revisit the original study to internally validate the proposed arginine-stimulated copeptin cut-offs of > 5.2pmol/L (high specificity cut-off with > 90% specificity for primary polydipsia) and ≤ 3.0 pmol/L (high specificity cut-off with > 90% specificity for AVP deficiency).
Findings: In total, 96 patients were included between May 2013 and June 2018: n = 38 [40%] with AVP deficiency and n = 58 [60%] with primary polydipsia. At 60 min after arginine infusion, a copeptin level ≤ 3.0 pmol/L showed a specificity of 95% (95% CI: 0.88-1.00) for AVP deficiency, while a copeptin level > 5.2 pmol/L demonstrated a specificity of 97% (95% CI: 0.92-1.00) for primary polydipsia. The ≤ 3.0 pmol/L cut-off accurately identified 71% (n = 27/38) of patients with AVP deficiency, and the > 5.2 pmol/L cut-off correctly identified 69% (n = 40/58) of patients with primary polydipsia.
Interpretation: This analysis validates two new copeptin cut-offs of the arginine stimulation test to distinguish AVP deficiency from primary polydipsia: >5.2 pmol/L for high specificity in diagnosing primary polydipsia and ≤ 3.0 pmol/L for high specificity in diagnosing AVP deficiency. These thresholds might offer a practical initial alternative to hypertonic saline testing.
期刊介绍:
Pituitary is an international publication devoted to basic and clinical aspects of the pituitary gland. It is designed to publish original, high quality research in both basic and pituitary function as well as clinical pituitary disease.
The journal considers:
Biology of Pituitary Tumors
Mechanisms of Pituitary Hormone Secretion
Regulation of Pituitary Function
Prospective Clinical Studies of Pituitary Disease
Critical Basic and Clinical Reviews
Pituitary is directed at basic investigators, physiologists, clinical adult and pediatric endocrinologists, neurosurgeons and reproductive endocrinologists interested in the broad field of the pituitary and its disorders. The Editorial Board has been drawn from international experts in basic and clinical endocrinology. The journal offers a rapid turnaround time for review of manuscripts, and the high standard of the journal is maintained by a selective peer-review process which aims to publish only the highest quality manuscripts. Pituitary will foster the publication of creative scholarship as it pertains to the pituitary and will provide a forum for basic scientists and clinicians to publish their high quality pituitary-related work.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


