Sayoni Sengupta, Parthasarathi Bhattacharyya, Aniruddha De, Sayanti Karmakar, Wrick Chakraborty, Dipanjan Saha
{"title":"COPD-PH和ILD-PH的血流动力学和运动后恢复反应:评估。","authors":"Sayoni Sengupta, Parthasarathi Bhattacharyya, Aniruddha De, Sayanti Karmakar, Wrick Chakraborty, Dipanjan Saha","doi":"10.4103/lungindia.lungindia_213_24","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Chronic lung disease (CLD) from either airway obstruction or parenchymal affections can lead to secondary pulmonary hypertension. It may be interesting to compare the two types of CLD-PH.</p><p><strong>Methods: </strong>Subjects of CLD were first evaluated for the primary category of disease with chest X-ray, HRCT chest, spirometry, and DLCO (diffusion capacity) and then for the presence of PH through exercise of the institutional clinic-radio-echocardiographic algorithm. Those qualifying as either unmixed restrictive (ILD) or COPD (chronic obstructive airway disease) with PH underwent two-chair test for assessment of post-exercise recovery response. The two groups were compared on available parameters.</p><p><strong>Results: </strong>The patients with COPD-PH were significantly older with similar FVC and DLCO compared to ILD-PH. In two-chair test, the maximum pulse rate and the desat-max were significantly worse (108.68 ± 1 5.46 vs 101.33 ± 12.62, P = 0.002, and - 5.68 ± 4.78 vs - 3.71 ± 2.73, P = 0.006) for the ILD-PH patients. The ILD-PH sufferers also demonstrated a lower TAPSE (21.16 ± 3.11 vs 22.59 ± 2.71; P-0.001) and a higher calculated mean pulmonary artery pressure (32.00 ± 7.54 vs 30.64 ± 4.22 vs, P = 0.05) compared to the subjects with COPD-PH. The other right ventricular systolic functional parameters [systolic excursion velocity (S-prime), right ventricular free wall global longitudinal strain, systolic pulmonary arterial pressure, tricuspid regurgitation jet velocity] supported the trend.</p><p><strong>Conclusion: </strong>The ILD-PH patients show relatively higher PH with lower right ventricular systolic function than COPD-PH.</p>","PeriodicalId":47462,"journal":{"name":"Lung India","volume":"42 3","pages":"225-230"},"PeriodicalIF":1.2000,"publicationDate":"2025-05-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12097658/pdf/","citationCount":"0","resultStr":"{\"title\":\"Haemodynamics and post-exercise recovery response in COPD-PH and ILD-PH: An appraisal.\",\"authors\":\"Sayoni Sengupta, Parthasarathi Bhattacharyya, Aniruddha De, Sayanti Karmakar, Wrick Chakraborty, Dipanjan Saha\",\"doi\":\"10.4103/lungindia.lungindia_213_24\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Chronic lung disease (CLD) from either airway obstruction or parenchymal affections can lead to secondary pulmonary hypertension. It may be interesting to compare the two types of CLD-PH.</p><p><strong>Methods: </strong>Subjects of CLD were first evaluated for the primary category of disease with chest X-ray, HRCT chest, spirometry, and DLCO (diffusion capacity) and then for the presence of PH through exercise of the institutional clinic-radio-echocardiographic algorithm. Those qualifying as either unmixed restrictive (ILD) or COPD (chronic obstructive airway disease) with PH underwent two-chair test for assessment of post-exercise recovery response. The two groups were compared on available parameters.</p><p><strong>Results: </strong>The patients with COPD-PH were significantly older with similar FVC and DLCO compared to ILD-PH. In two-chair test, the maximum pulse rate and the desat-max were significantly worse (108.68 ± 1 5.46 vs 101.33 ± 12.62, P = 0.002, and - 5.68 ± 4.78 vs - 3.71 ± 2.73, P = 0.006) for the ILD-PH patients. The ILD-PH sufferers also demonstrated a lower TAPSE (21.16 ± 3.11 vs 22.59 ± 2.71; P-0.001) and a higher calculated mean pulmonary artery pressure (32.00 ± 7.54 vs 30.64 ± 4.22 vs, P = 0.05) compared to the subjects with COPD-PH. The other right ventricular systolic functional parameters [systolic excursion velocity (S-prime), right ventricular free wall global longitudinal strain, systolic pulmonary arterial pressure, tricuspid regurgitation jet velocity] supported the trend.</p><p><strong>Conclusion: </strong>The ILD-PH patients show relatively higher PH with lower right ventricular systolic function than COPD-PH.</p>\",\"PeriodicalId\":47462,\"journal\":{\"name\":\"Lung India\",\"volume\":\"42 3\",\"pages\":\"225-230\"},\"PeriodicalIF\":1.2000,\"publicationDate\":\"2025-05-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12097658/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Lung India\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.4103/lungindia.lungindia_213_24\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/4/29 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q4\",\"JCRName\":\"RESPIRATORY SYSTEM\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Lung India","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4103/lungindia.lungindia_213_24","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/4/29 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"RESPIRATORY SYSTEM","Score":null,"Total":0}
引用次数: 0
摘要
背景:由气道阻塞或实质病变引起的慢性肺部疾病(CLD)可导致继发性肺动脉高压。比较两种类型的CLD-PH可能会很有趣。方法:首先通过胸部x线、HRCT胸部、肺活量测定和DLCO(扩散能力)评估CLD患者的主要疾病类型,然后通过临床-超声心动图算法评估PH的存在。患有非混合性限制性(ILD)或慢性阻塞性气道疾病(COPD)的患者接受双椅试验,以评估运动后恢复反应。比较两组可用参数。结果:COPD-PH患者年龄明显大于ILD-PH患者,FVC和DLCO相似。在双椅试验中,ILD-PH患者的最大脉搏率和最大脉搏值(desat-max)明显差(108.68±1.546 vs 101.33±12.62,P = 0.002, - 5.68±4.78 vs - 3.71±2.73,P = 0.006)。ILD-PH患者也表现出较低的TAPSE(21.16±3.11 vs 22.59±2.71;P = 0.001),与COPD-PH患者相比,计算的平均肺动脉压更高(32.00±7.54 vs 30.64±4.22 vs, P = 0.05)。其他右心室收缩功能参数[收缩偏移速度(S-prime),右心室自由壁整体纵向应变,收缩期肺动脉压,三尖瓣反流射流速度]支持这一趋势。结论:与COPD-PH相比,ILD-PH患者PH值较高,右心室收缩功能较低。
Haemodynamics and post-exercise recovery response in COPD-PH and ILD-PH: An appraisal.
Background: Chronic lung disease (CLD) from either airway obstruction or parenchymal affections can lead to secondary pulmonary hypertension. It may be interesting to compare the two types of CLD-PH.
Methods: Subjects of CLD were first evaluated for the primary category of disease with chest X-ray, HRCT chest, spirometry, and DLCO (diffusion capacity) and then for the presence of PH through exercise of the institutional clinic-radio-echocardiographic algorithm. Those qualifying as either unmixed restrictive (ILD) or COPD (chronic obstructive airway disease) with PH underwent two-chair test for assessment of post-exercise recovery response. The two groups were compared on available parameters.
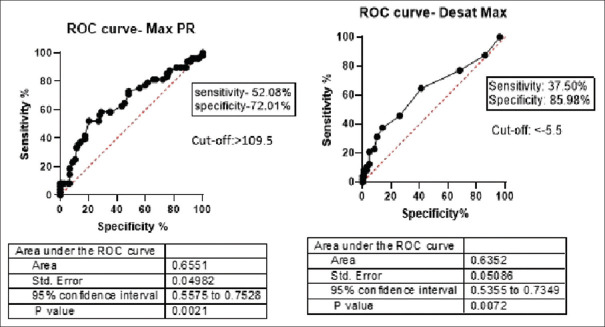
Results: The patients with COPD-PH were significantly older with similar FVC and DLCO compared to ILD-PH. In two-chair test, the maximum pulse rate and the desat-max were significantly worse (108.68 ± 1 5.46 vs 101.33 ± 12.62, P = 0.002, and - 5.68 ± 4.78 vs - 3.71 ± 2.73, P = 0.006) for the ILD-PH patients. The ILD-PH sufferers also demonstrated a lower TAPSE (21.16 ± 3.11 vs 22.59 ± 2.71; P-0.001) and a higher calculated mean pulmonary artery pressure (32.00 ± 7.54 vs 30.64 ± 4.22 vs, P = 0.05) compared to the subjects with COPD-PH. The other right ventricular systolic functional parameters [systolic excursion velocity (S-prime), right ventricular free wall global longitudinal strain, systolic pulmonary arterial pressure, tricuspid regurgitation jet velocity] supported the trend.
Conclusion: The ILD-PH patients show relatively higher PH with lower right ventricular systolic function than COPD-PH.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


