Maggie E Horn, Steven Z George, Anna Giczewska, Brooke Alhanti, Irene L Tanner, Michael P Bolognesi
{"title":"髋关节、膝关节和肩部全关节置换术后的不良事件、处方药和费用的比较:一项回顾性队列研究。","authors":"Maggie E Horn, Steven Z George, Anna Giczewska, Brooke Alhanti, Irene L Tanner, Michael P Bolognesi","doi":"10.1186/s42836-025-00309-y","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Outcomes from Total Joint Arthroplasty (TJA) are variable but generally favorable. However, the literature is lacking regarding direct comparisons of important outcomes across TJA sites. Such comparisons are of paramount importance to informing future bundled care reform and patient optimization. Thus, we compared the rates of adverse events, filled prescriptions, and costs at 90 days and 365 days after TJA for knee, hip, and shoulder patients.</p><p><strong>Methods: </strong>We conducted a retrospective cohort study of multi-payor claims data with patients (n = 2416) who underwent hip (n = 909), knee (n = 1250), or shoulder (n = 257) TJA within an academic health system. Univariable and multivariable logistic regression models were used to assess the association between the TJA surgical site and adverse events (i.e., medical and surgical complications) and prescriptions filled. Univariable and multivariable gamma regression models were used to assess the association between the TJA surgical site and total cost and surgical episode cost.</p><p><strong>Results: </strong>In all regression models, the hip location was used as the reference group. There were no differences in the adjusted odds of medical complications between the TJA surgical sites after adjusting for confounders at 90 days or 365 days. For surgical complications, the adjusted odds were 2.66 times higher in the knee (P < 0.001) and 4.48 times higher in the shoulder (P < 0.001) at 90 days. At 365 days, the odds were 2.54 times higher in the knee (P < 0.001) and 4.10 times higher in the shoulder (P < 0.001). There was an increase in the adjusted odds of antiepileptic and NSAIDS being filled in knee and shoulder patients compared to hip patients at 31-90 days (both P < 0.001). At 0-365 days, knee patients had increased adjusted odds of filled antibiotic (P = 0.032), antiepileptic (P = 0.001), and opioid (P = 0.005) prescriptions compared to hip patients, while shoulder patients only increased odds of antiepileptic (P = 0.028). Lastly, in adjusted models, both the knee and shoulder had a significant increase in total health system costs, with a 9% and 14% increase in cost, respectively (P < 0.01).</p><p><strong>Conclusion: </strong>Patients undergoing TKA and TSA may have an increased risk for surgical complications and longer-term opioid prescriptions (TKA only) compared to those undergoing THA. Collectively, these results can inform future population-based approaches to managing osteoarthritis care pathways or reimbursement policies for TJA across multiple joint sites.</p>","PeriodicalId":52831,"journal":{"name":"Arthroplasty","volume":"7 1","pages":"24"},"PeriodicalIF":4.3000,"publicationDate":"2025-05-06","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12054235/pdf/","citationCount":"0","resultStr":"{\"title\":\"Comparison of adverse events, prescription medication, and costs after hip, knee, and shoulder total joint arthroplasty: a retrospective cohort study.\",\"authors\":\"Maggie E Horn, Steven Z George, Anna Giczewska, Brooke Alhanti, Irene L Tanner, Michael P Bolognesi\",\"doi\":\"10.1186/s42836-025-00309-y\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Outcomes from Total Joint Arthroplasty (TJA) are variable but generally favorable. However, the literature is lacking regarding direct comparisons of important outcomes across TJA sites. Such comparisons are of paramount importance to informing future bundled care reform and patient optimization. Thus, we compared the rates of adverse events, filled prescriptions, and costs at 90 days and 365 days after TJA for knee, hip, and shoulder patients.</p><p><strong>Methods: </strong>We conducted a retrospective cohort study of multi-payor claims data with patients (n = 2416) who underwent hip (n = 909), knee (n = 1250), or shoulder (n = 257) TJA within an academic health system. Univariable and multivariable logistic regression models were used to assess the association between the TJA surgical site and adverse events (i.e., medical and surgical complications) and prescriptions filled. Univariable and multivariable gamma regression models were used to assess the association between the TJA surgical site and total cost and surgical episode cost.</p><p><strong>Results: </strong>In all regression models, the hip location was used as the reference group. There were no differences in the adjusted odds of medical complications between the TJA surgical sites after adjusting for confounders at 90 days or 365 days. For surgical complications, the adjusted odds were 2.66 times higher in the knee (P < 0.001) and 4.48 times higher in the shoulder (P < 0.001) at 90 days. At 365 days, the odds were 2.54 times higher in the knee (P < 0.001) and 4.10 times higher in the shoulder (P < 0.001). There was an increase in the adjusted odds of antiepileptic and NSAIDS being filled in knee and shoulder patients compared to hip patients at 31-90 days (both P < 0.001). At 0-365 days, knee patients had increased adjusted odds of filled antibiotic (P = 0.032), antiepileptic (P = 0.001), and opioid (P = 0.005) prescriptions compared to hip patients, while shoulder patients only increased odds of antiepileptic (P = 0.028). Lastly, in adjusted models, both the knee and shoulder had a significant increase in total health system costs, with a 9% and 14% increase in cost, respectively (P < 0.01).</p><p><strong>Conclusion: </strong>Patients undergoing TKA and TSA may have an increased risk for surgical complications and longer-term opioid prescriptions (TKA only) compared to those undergoing THA. Collectively, these results can inform future population-based approaches to managing osteoarthritis care pathways or reimbursement policies for TJA across multiple joint sites.</p>\",\"PeriodicalId\":52831,\"journal\":{\"name\":\"Arthroplasty\",\"volume\":\"7 1\",\"pages\":\"24\"},\"PeriodicalIF\":4.3000,\"publicationDate\":\"2025-05-06\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12054235/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Arthroplasty\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1186/s42836-025-00309-y\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"ORTHOPEDICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Arthroplasty","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s42836-025-00309-y","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
Comparison of adverse events, prescription medication, and costs after hip, knee, and shoulder total joint arthroplasty: a retrospective cohort study.
Background: Outcomes from Total Joint Arthroplasty (TJA) are variable but generally favorable. However, the literature is lacking regarding direct comparisons of important outcomes across TJA sites. Such comparisons are of paramount importance to informing future bundled care reform and patient optimization. Thus, we compared the rates of adverse events, filled prescriptions, and costs at 90 days and 365 days after TJA for knee, hip, and shoulder patients.
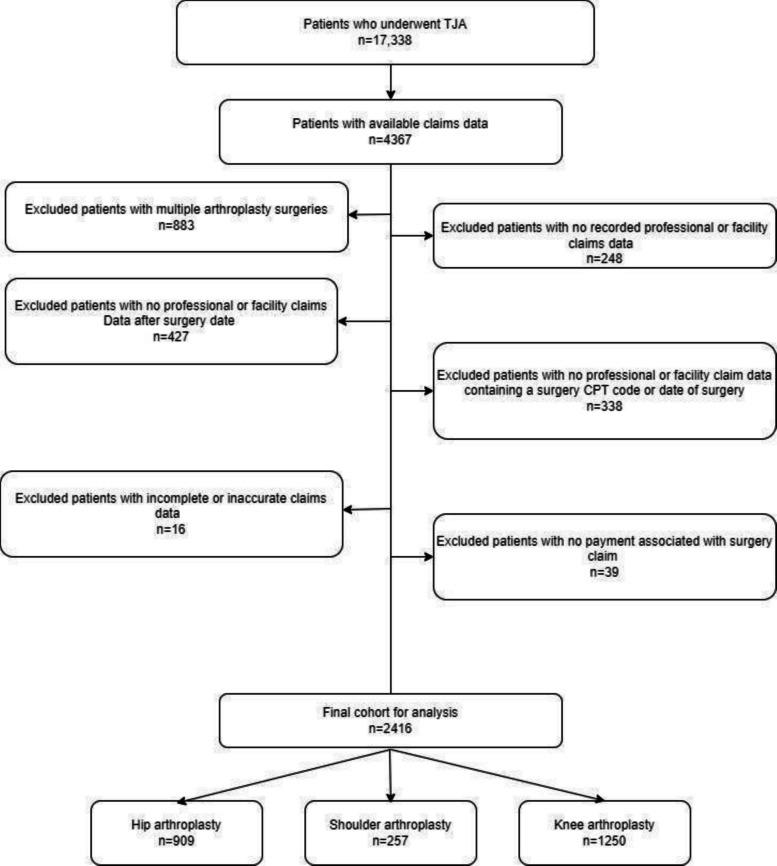
Methods: We conducted a retrospective cohort study of multi-payor claims data with patients (n = 2416) who underwent hip (n = 909), knee (n = 1250), or shoulder (n = 257) TJA within an academic health system. Univariable and multivariable logistic regression models were used to assess the association between the TJA surgical site and adverse events (i.e., medical and surgical complications) and prescriptions filled. Univariable and multivariable gamma regression models were used to assess the association between the TJA surgical site and total cost and surgical episode cost.
Results: In all regression models, the hip location was used as the reference group. There were no differences in the adjusted odds of medical complications between the TJA surgical sites after adjusting for confounders at 90 days or 365 days. For surgical complications, the adjusted odds were 2.66 times higher in the knee (P < 0.001) and 4.48 times higher in the shoulder (P < 0.001) at 90 days. At 365 days, the odds were 2.54 times higher in the knee (P < 0.001) and 4.10 times higher in the shoulder (P < 0.001). There was an increase in the adjusted odds of antiepileptic and NSAIDS being filled in knee and shoulder patients compared to hip patients at 31-90 days (both P < 0.001). At 0-365 days, knee patients had increased adjusted odds of filled antibiotic (P = 0.032), antiepileptic (P = 0.001), and opioid (P = 0.005) prescriptions compared to hip patients, while shoulder patients only increased odds of antiepileptic (P = 0.028). Lastly, in adjusted models, both the knee and shoulder had a significant increase in total health system costs, with a 9% and 14% increase in cost, respectively (P < 0.01).
Conclusion: Patients undergoing TKA and TSA may have an increased risk for surgical complications and longer-term opioid prescriptions (TKA only) compared to those undergoing THA. Collectively, these results can inform future population-based approaches to managing osteoarthritis care pathways or reimbursement policies for TJA across multiple joint sites.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


