Jung Eun Han, Soyeon Yoo, Sang Ah Lee, Gwanpyo Koh
{"title":"双侧肾上腺腺瘤伴双侧肾上腺自主分泌皮质醇和左肾上腺自主分泌醛固酮:1例报告。","authors":"Jung Eun Han, Soyeon Yoo, Sang Ah Lee, Gwanpyo Koh","doi":"10.12701/jyms.2025.42.33","DOIUrl":null,"url":null,"abstract":"<p><p>Primary aldosteronism (PA) is the most common cause of secondary hypertension and increases the morbidity and mortality associated with cardiovascular diseases. When PA coexists with autonomous cortisol secretion (ACS), the cardiovascular risk increases significantly, especially in cases of bilateral adrenal adenomas with asymmetric hormone secretion, which poses diagnostic and therapeutic challenges. A 50-year-old female presented with hypertension and hypokalemia. PA was diagnosed based on elevated aldosterone levels, suppressed plasma renin activity, and the results of various dynamic endocrine tests. Imaging revealed bilateral adrenal adenomas, and adrenal venous sampling (AVS) confirmed aldosterone hypersecretion from the left adrenal gland and cortisol hypersecretion from both adrenal glands. The patient subsequently underwent left adrenalectomy, which resolved the aldosterone hypersecretion and normalized blood pressure and potassium levels. However, the cortisol hypersecretion persisted. This case highlights the importance of AVS in identifying the sources of hormone secretion and enabling targeted surgical treatment while avoiding bilateral adrenalectomy, which can lead to lifelong adrenal insufficiency. Comprehensive endocrine evaluation, including ACS assessment, in patients with PA is essential to help reduce the cardiovascular risks associated with PA and ACS and thus improve treatment outcomes.</p>","PeriodicalId":74020,"journal":{"name":"Journal of Yeungnam medical science","volume":"42 ","pages":"33"},"PeriodicalIF":1.4000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12303784/pdf/","citationCount":"0","resultStr":"{\"title\":\"Bilateral adrenal adenomas with autonomous cortisol secretion from both glands and autonomous aldosterone secretion from the left adrenal: a case report.\",\"authors\":\"Jung Eun Han, Soyeon Yoo, Sang Ah Lee, Gwanpyo Koh\",\"doi\":\"10.12701/jyms.2025.42.33\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Primary aldosteronism (PA) is the most common cause of secondary hypertension and increases the morbidity and mortality associated with cardiovascular diseases. When PA coexists with autonomous cortisol secretion (ACS), the cardiovascular risk increases significantly, especially in cases of bilateral adrenal adenomas with asymmetric hormone secretion, which poses diagnostic and therapeutic challenges. A 50-year-old female presented with hypertension and hypokalemia. PA was diagnosed based on elevated aldosterone levels, suppressed plasma renin activity, and the results of various dynamic endocrine tests. Imaging revealed bilateral adrenal adenomas, and adrenal venous sampling (AVS) confirmed aldosterone hypersecretion from the left adrenal gland and cortisol hypersecretion from both adrenal glands. The patient subsequently underwent left adrenalectomy, which resolved the aldosterone hypersecretion and normalized blood pressure and potassium levels. However, the cortisol hypersecretion persisted. This case highlights the importance of AVS in identifying the sources of hormone secretion and enabling targeted surgical treatment while avoiding bilateral adrenalectomy, which can lead to lifelong adrenal insufficiency. Comprehensive endocrine evaluation, including ACS assessment, in patients with PA is essential to help reduce the cardiovascular risks associated with PA and ACS and thus improve treatment outcomes.</p>\",\"PeriodicalId\":74020,\"journal\":{\"name\":\"Journal of Yeungnam medical science\",\"volume\":\"42 \",\"pages\":\"33\"},\"PeriodicalIF\":1.4000,\"publicationDate\":\"2025-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12303784/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Yeungnam medical science\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.12701/jyms.2025.42.33\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/4/28 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"MEDICINE, GENERAL & INTERNAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Yeungnam medical science","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.12701/jyms.2025.42.33","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/4/28 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
Bilateral adrenal adenomas with autonomous cortisol secretion from both glands and autonomous aldosterone secretion from the left adrenal: a case report.
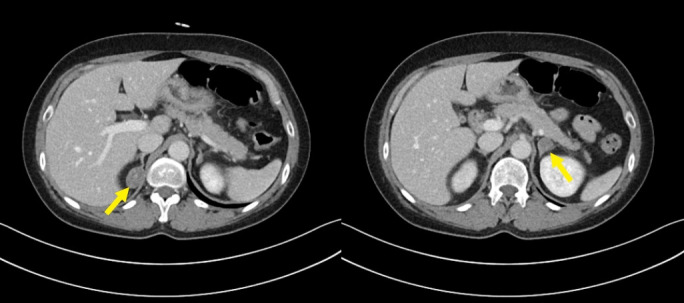
Primary aldosteronism (PA) is the most common cause of secondary hypertension and increases the morbidity and mortality associated with cardiovascular diseases. When PA coexists with autonomous cortisol secretion (ACS), the cardiovascular risk increases significantly, especially in cases of bilateral adrenal adenomas with asymmetric hormone secretion, which poses diagnostic and therapeutic challenges. A 50-year-old female presented with hypertension and hypokalemia. PA was diagnosed based on elevated aldosterone levels, suppressed plasma renin activity, and the results of various dynamic endocrine tests. Imaging revealed bilateral adrenal adenomas, and adrenal venous sampling (AVS) confirmed aldosterone hypersecretion from the left adrenal gland and cortisol hypersecretion from both adrenal glands. The patient subsequently underwent left adrenalectomy, which resolved the aldosterone hypersecretion and normalized blood pressure and potassium levels. However, the cortisol hypersecretion persisted. This case highlights the importance of AVS in identifying the sources of hormone secretion and enabling targeted surgical treatment while avoiding bilateral adrenalectomy, which can lead to lifelong adrenal insufficiency. Comprehensive endocrine evaluation, including ACS assessment, in patients with PA is essential to help reduce the cardiovascular risks associated with PA and ACS and thus improve treatment outcomes.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


