{"title":"探讨血小板聚集功能与血栓性卒中患者服用普拉格雷和氯吡格雷后疗效和安全性的关系:一项对PRASTRO合并研究的事后分析","authors":"Kazumi Kimura, Masahiro Kamouchi, Yuji Matsumaru, Tetsuya Kimura, Rina Katsuro, Jun Hosokawa, Takanari Kitazono","doi":"10.1007/s11239-025-03093-3","DOIUrl":null,"url":null,"abstract":"<p><p>The P2Y12 receptor inhibitor prasugrel was approved for thrombotic stroke in Japan following the phase 3 clinical trials PRASTRO-I, -II, and -III. However, correlations between elevated platelet reaction unit (PRU) and ischemic event risk remain unclear. This post hoc integrated analysis of PRASTRO-I, -II, and -III assessed the relationships of PRU with efficacy and safety outcomes, and risk factors for high PRU (HPR). Patients from PRASTRO-I, -II, and -III receiving prasugrel or clopidogrel and with PRU values at 4 and 24 weeks after treatment initiation were included. The primary endpoint was PRU at 4 weeks; secondary endpoints included cumulative incidence of ischemic and bleeding events from study drug initiation to 48 weeks. Exploratory univariate and multivariate analyses were conducted to identify HPR risk factors. Of 2688 patients analyzed, 2595 and 2434 had PRU values available at 4 and 24 weeks, respectively. Mean PRU was numerically lower with prasugrel than clopidogrel at 4 weeks (151.3 vs. 195.4) and 24 weeks (143.8 vs. 188.0). CYP2C19 polymorphisms affected PRU at 4 and 24 weeks with clopidogrel but not with prasugrel. PRU at 4 weeks did not predict ischemic and bleeding event incidence up to 48 weeks. The CYP2C19 poor metabolizer phenotype was the strongest HPR risk factor. PRU values at 4 and 24 weeks were numerically lower with prasugrel and unaffected by CYP2C19 genetic polymorphisms. Further research is needed to clarify the relationship of PRU with ischemic and bleeding events.</p>","PeriodicalId":17546,"journal":{"name":"Journal of Thrombosis and Thrombolysis","volume":"58 4","pages":"547-555"},"PeriodicalIF":2.2000,"publicationDate":"2025-04-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12043787/pdf/","citationCount":"0","resultStr":"{\"title\":\"Exploring the relationship of platelet aggregation function with efficacy and safety outcomes following the administration of prasugrel and clopidogrel in patients with thrombotic stroke: a post hoc analysis of PRASTRO pooled studies.\",\"authors\":\"Kazumi Kimura, Masahiro Kamouchi, Yuji Matsumaru, Tetsuya Kimura, Rina Katsuro, Jun Hosokawa, Takanari Kitazono\",\"doi\":\"10.1007/s11239-025-03093-3\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>The P2Y12 receptor inhibitor prasugrel was approved for thrombotic stroke in Japan following the phase 3 clinical trials PRASTRO-I, -II, and -III. However, correlations between elevated platelet reaction unit (PRU) and ischemic event risk remain unclear. This post hoc integrated analysis of PRASTRO-I, -II, and -III assessed the relationships of PRU with efficacy and safety outcomes, and risk factors for high PRU (HPR). Patients from PRASTRO-I, -II, and -III receiving prasugrel or clopidogrel and with PRU values at 4 and 24 weeks after treatment initiation were included. The primary endpoint was PRU at 4 weeks; secondary endpoints included cumulative incidence of ischemic and bleeding events from study drug initiation to 48 weeks. Exploratory univariate and multivariate analyses were conducted to identify HPR risk factors. Of 2688 patients analyzed, 2595 and 2434 had PRU values available at 4 and 24 weeks, respectively. Mean PRU was numerically lower with prasugrel than clopidogrel at 4 weeks (151.3 vs. 195.4) and 24 weeks (143.8 vs. 188.0). CYP2C19 polymorphisms affected PRU at 4 and 24 weeks with clopidogrel but not with prasugrel. PRU at 4 weeks did not predict ischemic and bleeding event incidence up to 48 weeks. The CYP2C19 poor metabolizer phenotype was the strongest HPR risk factor. PRU values at 4 and 24 weeks were numerically lower with prasugrel and unaffected by CYP2C19 genetic polymorphisms. Further research is needed to clarify the relationship of PRU with ischemic and bleeding events.</p>\",\"PeriodicalId\":17546,\"journal\":{\"name\":\"Journal of Thrombosis and Thrombolysis\",\"volume\":\"58 4\",\"pages\":\"547-555\"},\"PeriodicalIF\":2.2000,\"publicationDate\":\"2025-04-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12043787/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Thrombosis and Thrombolysis\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s11239-025-03093-3\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/4/14 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q2\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Thrombosis and Thrombolysis","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s11239-025-03093-3","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/4/14 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
摘要
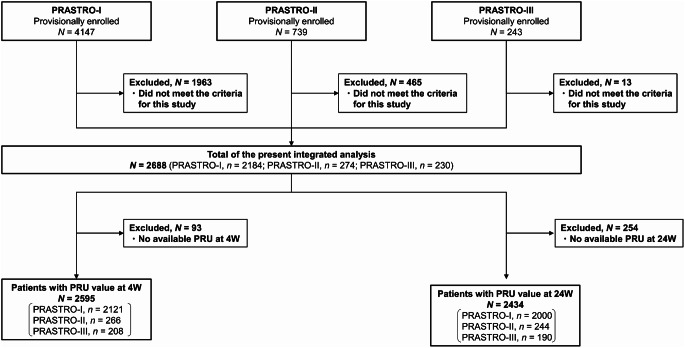
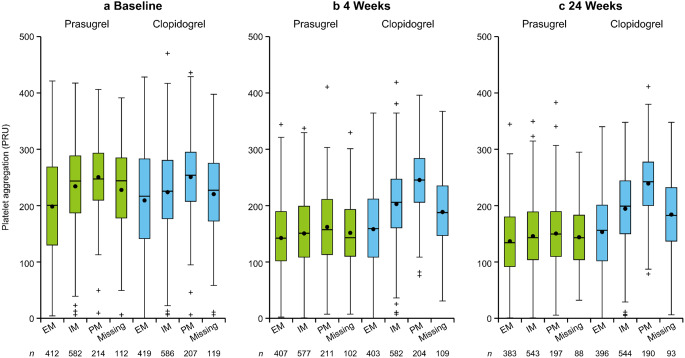
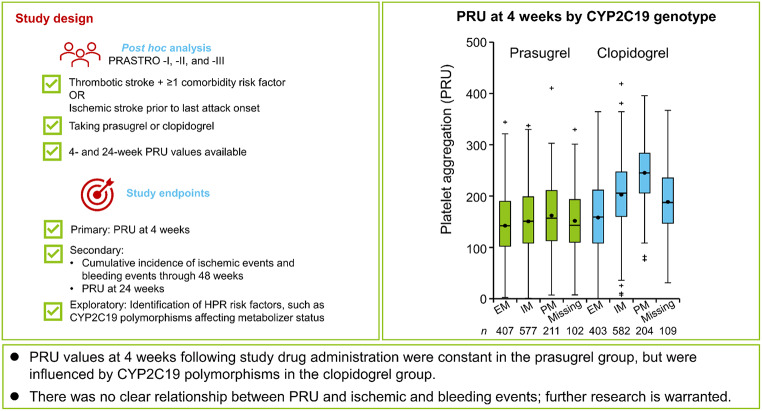
P2Y12受体抑制剂普拉格雷在日本通过PRASTRO-I、-II和-III期临床试验后被批准用于血栓性卒中。然而,血小板反应单位(PRU)升高与缺血性事件风险之间的相关性尚不清楚。这项对PRASTRO-I、-II和-III的事后综合分析评估了PRU与疗效和安全性结局以及高PRU (HPR)的危险因素之间的关系。prastro - 1、-II和-III患者接受普拉格雷或氯吡格雷治疗,并在治疗开始后4周和24周具有PRU值。主要终点是4周时的PRU;次要终点包括从研究药物开始到48周的缺血性和出血事件的累积发生率。进行探索性单因素和多因素分析以确定HPR的危险因素。在分析的2688例患者中,分别有2595例和2434例在4周和24周时可获得PRU值。在4周(151.3 vs. 195.4)和24周(143.8 vs. 188.0)时,普拉格雷的平均PRU数值低于氯吡格雷。CYP2C19多态性影响氯吡格雷治疗4周和24周的PRU,而普拉格雷治疗不影响PRU。4周PRU不能预测48周的缺血和出血事件的发生率。CYP2C19代谢不良表型是最强的HPR危险因素。4周和24周时PRU值在普拉格雷组数值较低,且不受CYP2C19基因多态性的影响。PRU与缺血性和出血事件的关系有待进一步研究。
Exploring the relationship of platelet aggregation function with efficacy and safety outcomes following the administration of prasugrel and clopidogrel in patients with thrombotic stroke: a post hoc analysis of PRASTRO pooled studies.
The P2Y12 receptor inhibitor prasugrel was approved for thrombotic stroke in Japan following the phase 3 clinical trials PRASTRO-I, -II, and -III. However, correlations between elevated platelet reaction unit (PRU) and ischemic event risk remain unclear. This post hoc integrated analysis of PRASTRO-I, -II, and -III assessed the relationships of PRU with efficacy and safety outcomes, and risk factors for high PRU (HPR). Patients from PRASTRO-I, -II, and -III receiving prasugrel or clopidogrel and with PRU values at 4 and 24 weeks after treatment initiation were included. The primary endpoint was PRU at 4 weeks; secondary endpoints included cumulative incidence of ischemic and bleeding events from study drug initiation to 48 weeks. Exploratory univariate and multivariate analyses were conducted to identify HPR risk factors. Of 2688 patients analyzed, 2595 and 2434 had PRU values available at 4 and 24 weeks, respectively. Mean PRU was numerically lower with prasugrel than clopidogrel at 4 weeks (151.3 vs. 195.4) and 24 weeks (143.8 vs. 188.0). CYP2C19 polymorphisms affected PRU at 4 and 24 weeks with clopidogrel but not with prasugrel. PRU at 4 weeks did not predict ischemic and bleeding event incidence up to 48 weeks. The CYP2C19 poor metabolizer phenotype was the strongest HPR risk factor. PRU values at 4 and 24 weeks were numerically lower with prasugrel and unaffected by CYP2C19 genetic polymorphisms. Further research is needed to clarify the relationship of PRU with ischemic and bleeding events.
期刊介绍:
The Journal of Thrombosis and Thrombolysis is a long-awaited resource for contemporary cardiologists, hematologists, vascular medicine specialists and clinician-scientists actively involved in treatment decisions and clinical investigation of thrombotic disorders involving the cardiovascular and cerebrovascular systems. The principal focus of the Journal centers on the pathobiology of thrombosis and vascular disorders and the use of anticoagulants, platelet antagonists, cell-based therapies and interventions in scientific investigation, clinical-translational research and patient care.
The Journal will publish original work which emphasizes the interface between fundamental scientific principles and clinical investigation, stimulating an interdisciplinary and scholarly dialogue in thrombosis and vascular science. Published works will also define platforms for translational research, drug development, clinical trials and patient-directed applications. The Journal of Thrombosis and Thrombolysis'' integrated format will expand the reader''s knowledge base and provide important insights for both the investigation and direct clinical application of the most rapidly growing fields in medicine-thrombosis and vascular science.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


