Kati Sulin, Mikko Arvas, Suvi Toivonen, Katri Haimila, Jaana Mättö, Inna Sareneva, Riina Jernman, Anna Parhamaa, Susanna Sainio
{"title":"常规试管技术与自动凝胶微柱法产前抗体监测的比较。","authors":"Kati Sulin, Mikko Arvas, Suvi Toivonen, Katri Haimila, Jaana Mättö, Inna Sareneva, Riina Jernman, Anna Parhamaa, Susanna Sainio","doi":"10.1111/vox.70042","DOIUrl":null,"url":null,"abstract":"<p><strong>Background and objectives: </strong>Timely identification of pregnancies at risk of severe haemolytic disease of the fetus and newborn (HDFN) requires accurate and reproducible antibody titration. This study aimed to establish a critical titre for the gel microcolumn assay (GMA) corresponding to the critical titre of ≥16 for the conventional tube technique (CTT) and to evaluate GMA's suitability for routine antenatal antibody titration.</p><p><strong>Materials and methods: </strong>Altogether, 147 antenatal plasma samples with clinically significant antibodies were studied, including eight pregnancies requiring intrauterine transfusions (IUTs). Twofold serial dilution titres with CTT were made in parallel with automated GMA. Single-dose red blood cells were used with a concentration of 3.5% for CTT and 0.8% for GMA. The critical titre for GMA was compared with CTT as the gold standard.</p><p><strong>Results: </strong>GMA titres were on average 2.88 (95% confidence interval [CI]: 2.72-3.05) dilutions higher than CTT titres. At a CTT titre of 16, the sensitivity and specificity of GMA titration were maximum (94%, 95% CI: 81-99 and 92%, 95% CI: 85-96, respectively) at a titre of 128, but one of the eight fetuses (12.5%) requiring IUTs would have been missed. At a GMA titre of ≥64, sensitivity and specificity were 100% (95% CI: 100-100) and 77% (95% CI: 68-84) respectively, but the number of pregnancies requiring clinical monitoring more than doubled (2.5×).</p><p><strong>Conclusion: </strong>A GMA titre ≥64 could be considered a safe critical value for high-risk assessment. Despite being a fully automated method benefiting the screening laboratory, the additional workload and costs caused by unnecessary monitoring at delivery hospitals were unacceptable.</p>","PeriodicalId":23631,"journal":{"name":"Vox Sanguinis","volume":" ","pages":"708-713"},"PeriodicalIF":1.6000,"publicationDate":"2025-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12286668/pdf/","citationCount":"0","resultStr":"{\"title\":\"Comparison of conventional tube technique with automated gel microcolumn assay for antenatal antibody monitoring.\",\"authors\":\"Kati Sulin, Mikko Arvas, Suvi Toivonen, Katri Haimila, Jaana Mättö, Inna Sareneva, Riina Jernman, Anna Parhamaa, Susanna Sainio\",\"doi\":\"10.1111/vox.70042\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background and objectives: </strong>Timely identification of pregnancies at risk of severe haemolytic disease of the fetus and newborn (HDFN) requires accurate and reproducible antibody titration. This study aimed to establish a critical titre for the gel microcolumn assay (GMA) corresponding to the critical titre of ≥16 for the conventional tube technique (CTT) and to evaluate GMA's suitability for routine antenatal antibody titration.</p><p><strong>Materials and methods: </strong>Altogether, 147 antenatal plasma samples with clinically significant antibodies were studied, including eight pregnancies requiring intrauterine transfusions (IUTs). Twofold serial dilution titres with CTT were made in parallel with automated GMA. Single-dose red blood cells were used with a concentration of 3.5% for CTT and 0.8% for GMA. The critical titre for GMA was compared with CTT as the gold standard.</p><p><strong>Results: </strong>GMA titres were on average 2.88 (95% confidence interval [CI]: 2.72-3.05) dilutions higher than CTT titres. At a CTT titre of 16, the sensitivity and specificity of GMA titration were maximum (94%, 95% CI: 81-99 and 92%, 95% CI: 85-96, respectively) at a titre of 128, but one of the eight fetuses (12.5%) requiring IUTs would have been missed. At a GMA titre of ≥64, sensitivity and specificity were 100% (95% CI: 100-100) and 77% (95% CI: 68-84) respectively, but the number of pregnancies requiring clinical monitoring more than doubled (2.5×).</p><p><strong>Conclusion: </strong>A GMA titre ≥64 could be considered a safe critical value for high-risk assessment. Despite being a fully automated method benefiting the screening laboratory, the additional workload and costs caused by unnecessary monitoring at delivery hospitals were unacceptable.</p>\",\"PeriodicalId\":23631,\"journal\":{\"name\":\"Vox Sanguinis\",\"volume\":\" \",\"pages\":\"708-713\"},\"PeriodicalIF\":1.6000,\"publicationDate\":\"2025-07-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12286668/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Vox Sanguinis\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1111/vox.70042\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/4/29 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"HEMATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Vox Sanguinis","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1111/vox.70042","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/4/29 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"HEMATOLOGY","Score":null,"Total":0}
Comparison of conventional tube technique with automated gel microcolumn assay for antenatal antibody monitoring.
Background and objectives: Timely identification of pregnancies at risk of severe haemolytic disease of the fetus and newborn (HDFN) requires accurate and reproducible antibody titration. This study aimed to establish a critical titre for the gel microcolumn assay (GMA) corresponding to the critical titre of ≥16 for the conventional tube technique (CTT) and to evaluate GMA's suitability for routine antenatal antibody titration.
Materials and methods: Altogether, 147 antenatal plasma samples with clinically significant antibodies were studied, including eight pregnancies requiring intrauterine transfusions (IUTs). Twofold serial dilution titres with CTT were made in parallel with automated GMA. Single-dose red blood cells were used with a concentration of 3.5% for CTT and 0.8% for GMA. The critical titre for GMA was compared with CTT as the gold standard.
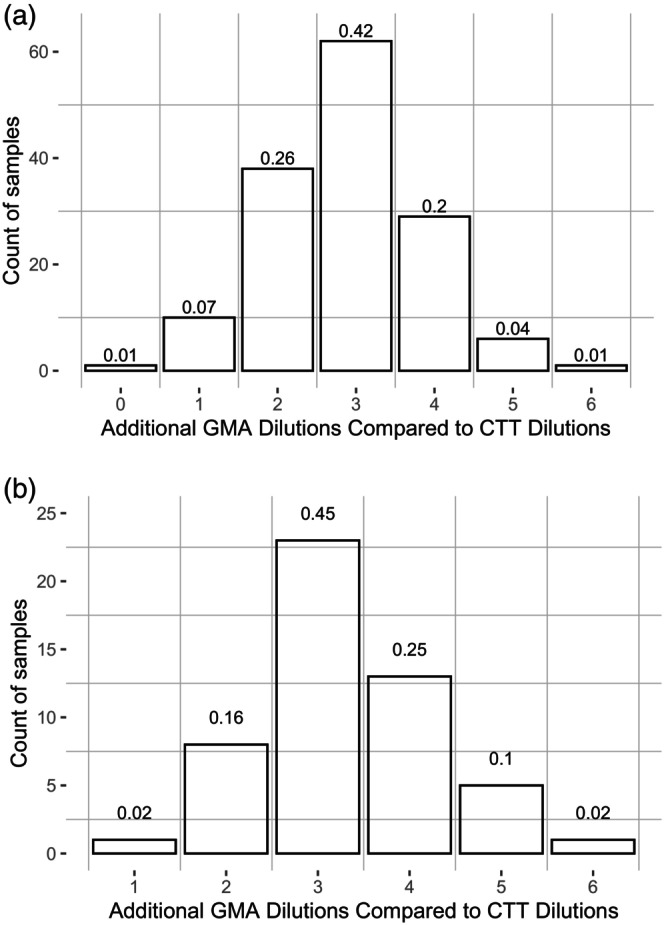
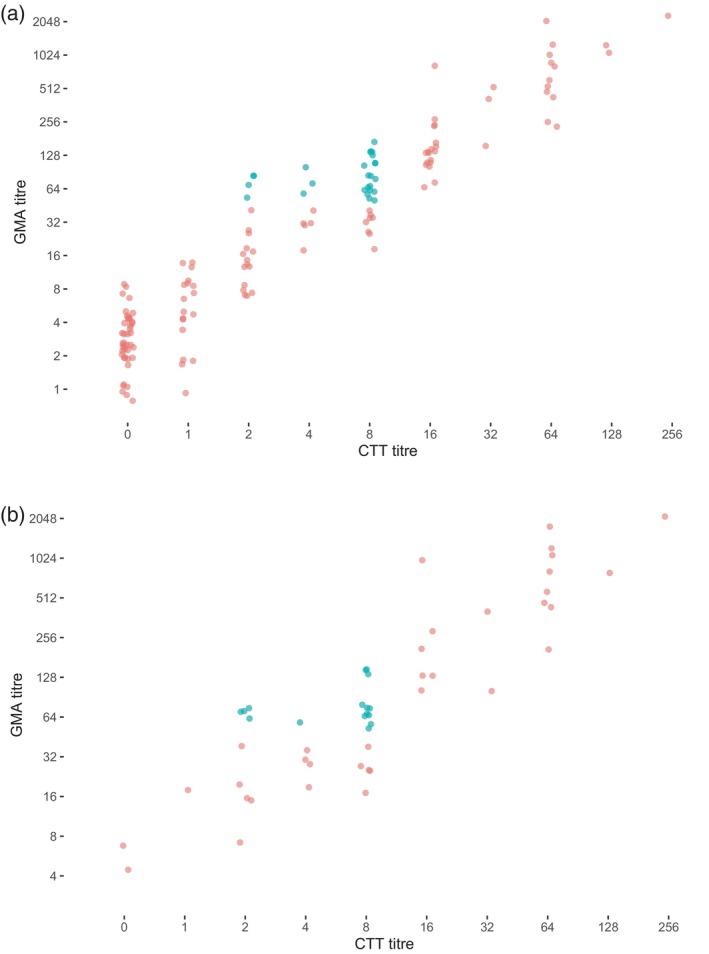
Results: GMA titres were on average 2.88 (95% confidence interval [CI]: 2.72-3.05) dilutions higher than CTT titres. At a CTT titre of 16, the sensitivity and specificity of GMA titration were maximum (94%, 95% CI: 81-99 and 92%, 95% CI: 85-96, respectively) at a titre of 128, but one of the eight fetuses (12.5%) requiring IUTs would have been missed. At a GMA titre of ≥64, sensitivity and specificity were 100% (95% CI: 100-100) and 77% (95% CI: 68-84) respectively, but the number of pregnancies requiring clinical monitoring more than doubled (2.5×).
Conclusion: A GMA titre ≥64 could be considered a safe critical value for high-risk assessment. Despite being a fully automated method benefiting the screening laboratory, the additional workload and costs caused by unnecessary monitoring at delivery hospitals were unacceptable.
期刊介绍:
Vox Sanguinis reports on important, novel developments in transfusion medicine. Original papers, reviews and international fora are published on all aspects of blood transfusion and tissue transplantation, comprising five main sections:
1) Transfusion - Transmitted Disease and its Prevention:
Identification and epidemiology of infectious agents transmissible by blood;
Bacterial contamination of blood components;
Donor recruitment and selection methods;
Pathogen inactivation.
2) Blood Component Collection and Production:
Blood collection methods and devices (including apheresis);
Plasma fractionation techniques and plasma derivatives;
Preparation of labile blood components;
Inventory management;
Hematopoietic progenitor cell collection and storage;
Collection and storage of tissues;
Quality management and good manufacturing practice;
Automation and information technology.
3) Transfusion Medicine and New Therapies:
Transfusion thresholds and audits;
Haemovigilance;
Clinical trials regarding appropriate haemotherapy;
Non-infectious adverse affects of transfusion;
Therapeutic apheresis;
Support of transplant patients;
Gene therapy and immunotherapy.
4) Immunohaematology and Immunogenetics:
Autoimmunity in haematology;
Alloimmunity of blood;
Pre-transfusion testing;
Immunodiagnostics;
Immunobiology;
Complement in immunohaematology;
Blood typing reagents;
Genetic markers of blood cells and serum proteins: polymorphisms and function;
Genetic markers and disease;
Parentage testing and forensic immunohaematology.
5) Cellular Therapy:
Cell-based therapies;
Stem cell sources;
Stem cell processing and storage;
Stem cell products;
Stem cell plasticity;
Regenerative medicine with cells;
Cellular immunotherapy;
Molecular therapy;
Gene therapy.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


