{"title":"爱泼斯坦-巴尔病毒不匹配成人和儿童实体器官移植受者全血dna血症的发生率和时间","authors":"Catherine Burton, Curtis Mabilangan, Jutta Preiksaitis","doi":"10.1111/tid.70042","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Epstein-Barr virus (EBV) viral load (VL) monitoring is recommended post-transplant for EBV-mismatched (donor EBV seropositive/recipient EBV seronegative) solid organ transplant (SOT) recipients as a component of post-transplant lymphoproliferative disorder (PTLD) prevention, but the optimal frequency and timing of EBV VL monitoring remains unknown.</p><p><strong>Methods: </strong>In this retrospective cohort study, we investigated the incidence and timing of whole blood EBV DNAemia in EBV-mismatched adult and pediatric SOT recipients, who had EBV VL monitoring as part of a pre-emptive approach to PTLD prevention to optimize monitoring algorithms. We explored associations between donor-acquired EBV DNAemia (DA-EBV), defined as EBV DNAemia within 1 year post-transplant, and donor and recipient characteristics, and determined the proportion who developed PTLD.</p><p><strong>Results: </strong>We analyzed 257 D<sup>+</sup>/R<sup>-</sup> recipients (kidney n = 64, heart n = 75, liver n = 93, lung n = 25); 126/257 (49.0%) developed DA-EBV at a median of 83 days (Q1-Q3: 50-130 days) post-transplant. Incidence of DA-EBV varied by organ and was highest in liver (62.4%) and lowest in heart recipients (28.0%). PTLD was diagnosed in 38/257 (14.8%) EBV-mismatched recipients, 25/162 (15.4%) children, and 13/95 (13.7%) adults. DA-EBV was uncommon in recipients less than 6 months old (3/29, 10.3%) and among recipients less than 12 months with donors less than 12 months (2/29, 6.9%); possible mechanisms of protection other than recipient passive maternal antibody and false-positive donor serostatus are discussed.</p><p><strong>Conclusion: </strong>Monitoring for DA-EBV should be focused on months 2-6 post-transplant. Less frequent whole blood EBV VL monitoring is likely a safe option in recipients less than 6 months old and recipients 6-12 months old with donors less than 12 months old.</p>","PeriodicalId":23318,"journal":{"name":"Transplant Infectious Disease","volume":" ","pages":"e70042"},"PeriodicalIF":2.6000,"publicationDate":"2025-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12416345/pdf/","citationCount":"0","resultStr":"{\"title\":\"Incidence and Timing of Epstein-Barr Virus Whole Blood DNAemia in Epstein-Barr Virus-Mismatched Adult and Pediatric Solid Organ Transplant Recipients.\",\"authors\":\"Catherine Burton, Curtis Mabilangan, Jutta Preiksaitis\",\"doi\":\"10.1111/tid.70042\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Epstein-Barr virus (EBV) viral load (VL) monitoring is recommended post-transplant for EBV-mismatched (donor EBV seropositive/recipient EBV seronegative) solid organ transplant (SOT) recipients as a component of post-transplant lymphoproliferative disorder (PTLD) prevention, but the optimal frequency and timing of EBV VL monitoring remains unknown.</p><p><strong>Methods: </strong>In this retrospective cohort study, we investigated the incidence and timing of whole blood EBV DNAemia in EBV-mismatched adult and pediatric SOT recipients, who had EBV VL monitoring as part of a pre-emptive approach to PTLD prevention to optimize monitoring algorithms. We explored associations between donor-acquired EBV DNAemia (DA-EBV), defined as EBV DNAemia within 1 year post-transplant, and donor and recipient characteristics, and determined the proportion who developed PTLD.</p><p><strong>Results: </strong>We analyzed 257 D<sup>+</sup>/R<sup>-</sup> recipients (kidney n = 64, heart n = 75, liver n = 93, lung n = 25); 126/257 (49.0%) developed DA-EBV at a median of 83 days (Q1-Q3: 50-130 days) post-transplant. Incidence of DA-EBV varied by organ and was highest in liver (62.4%) and lowest in heart recipients (28.0%). PTLD was diagnosed in 38/257 (14.8%) EBV-mismatched recipients, 25/162 (15.4%) children, and 13/95 (13.7%) adults. DA-EBV was uncommon in recipients less than 6 months old (3/29, 10.3%) and among recipients less than 12 months with donors less than 12 months (2/29, 6.9%); possible mechanisms of protection other than recipient passive maternal antibody and false-positive donor serostatus are discussed.</p><p><strong>Conclusion: </strong>Monitoring for DA-EBV should be focused on months 2-6 post-transplant. Less frequent whole blood EBV VL monitoring is likely a safe option in recipients less than 6 months old and recipients 6-12 months old with donors less than 12 months old.</p>\",\"PeriodicalId\":23318,\"journal\":{\"name\":\"Transplant Infectious Disease\",\"volume\":\" \",\"pages\":\"e70042\"},\"PeriodicalIF\":2.6000,\"publicationDate\":\"2025-07-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12416345/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Transplant Infectious Disease\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1111/tid.70042\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/4/29 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"IMMUNOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Transplant Infectious Disease","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1111/tid.70042","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/4/29 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"IMMUNOLOGY","Score":null,"Total":0}
Incidence and Timing of Epstein-Barr Virus Whole Blood DNAemia in Epstein-Barr Virus-Mismatched Adult and Pediatric Solid Organ Transplant Recipients.
Background: Epstein-Barr virus (EBV) viral load (VL) monitoring is recommended post-transplant for EBV-mismatched (donor EBV seropositive/recipient EBV seronegative) solid organ transplant (SOT) recipients as a component of post-transplant lymphoproliferative disorder (PTLD) prevention, but the optimal frequency and timing of EBV VL monitoring remains unknown.
Methods: In this retrospective cohort study, we investigated the incidence and timing of whole blood EBV DNAemia in EBV-mismatched adult and pediatric SOT recipients, who had EBV VL monitoring as part of a pre-emptive approach to PTLD prevention to optimize monitoring algorithms. We explored associations between donor-acquired EBV DNAemia (DA-EBV), defined as EBV DNAemia within 1 year post-transplant, and donor and recipient characteristics, and determined the proportion who developed PTLD.
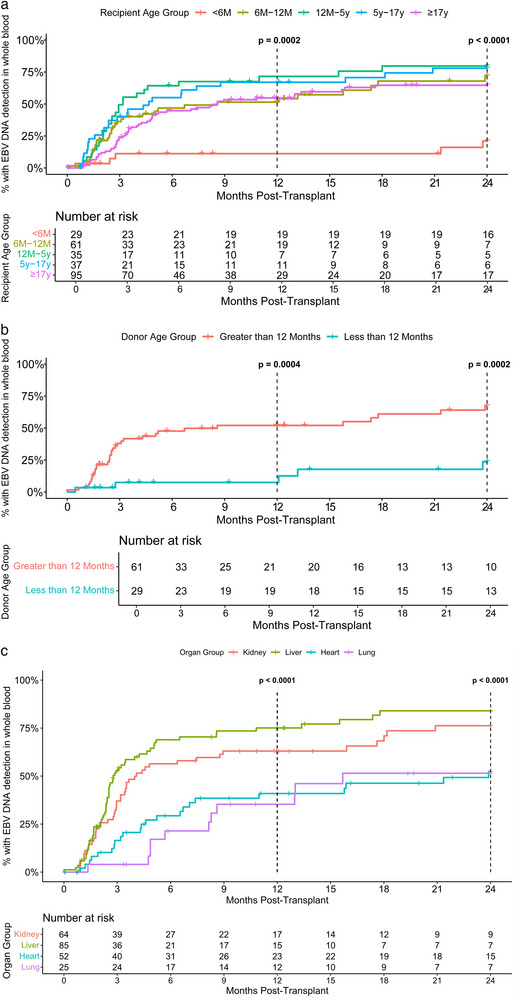
Results: We analyzed 257 D+/R- recipients (kidney n = 64, heart n = 75, liver n = 93, lung n = 25); 126/257 (49.0%) developed DA-EBV at a median of 83 days (Q1-Q3: 50-130 days) post-transplant. Incidence of DA-EBV varied by organ and was highest in liver (62.4%) and lowest in heart recipients (28.0%). PTLD was diagnosed in 38/257 (14.8%) EBV-mismatched recipients, 25/162 (15.4%) children, and 13/95 (13.7%) adults. DA-EBV was uncommon in recipients less than 6 months old (3/29, 10.3%) and among recipients less than 12 months with donors less than 12 months (2/29, 6.9%); possible mechanisms of protection other than recipient passive maternal antibody and false-positive donor serostatus are discussed.
Conclusion: Monitoring for DA-EBV should be focused on months 2-6 post-transplant. Less frequent whole blood EBV VL monitoring is likely a safe option in recipients less than 6 months old and recipients 6-12 months old with donors less than 12 months old.
期刊介绍:
Transplant Infectious Disease has been established as a forum for presenting the most current information on the prevention and treatment of infection complicating organ and bone marrow transplantation. The point of view of the journal is that infection and allograft rejection (or graft-versus-host disease) are closely intertwined, and that advances in one area will have immediate consequences on the other. The interaction of the transplant recipient with potential microbial invaders, the impact of immunosuppressive strategies on this interaction, and the effects of cytokines, growth factors, and chemokines liberated during the course of infections, rejection, or graft-versus-host disease are central to the interests and mission of this journal.
Transplant Infectious Disease is aimed at disseminating the latest information relevant to the infectious disease complications of transplantation to clinicians and scientists involved in bone marrow, kidney, liver, heart, lung, intestinal, and pancreatic transplantation. The infectious disease consequences and concerns regarding innovative transplant strategies, from novel immunosuppressive agents to xenotransplantation, are very much a concern of this journal. In addition, this journal feels a particular responsibility to inform primary care practitioners in the community, who increasingly are sharing the responsibility for the care of these patients, of the special considerations regarding the prevention and treatment of infection in transplant recipients. As exemplified by the international editorial board, articles are sought throughout the world that address both general issues and those of a more restricted geographic import.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


