Eung-Joon Lee, Han-Yeong Jeong, Jayoun Kim, Nan Hee Park, Min Kyoung Kang, Dongwhane Lee, Jinkwon Kim, Yo Han Jung, Sungwook Yu, Wook-Joo Kim, Han-Jin Cho, Kyungbok Lee, Tai Hwan Park, Mi Sun Oh, Ji Sung Lee, Joon-Tae Kim, Byung-Woo Yoon, Jong-Moo Park, Hee-Joon Bae, Keun-Hwa Jung
{"title":"血管内取栓时间对急性脑卒中治疗效果的评价。","authors":"Eung-Joon Lee, Han-Yeong Jeong, Jayoun Kim, Nan Hee Park, Min Kyoung Kang, Dongwhane Lee, Jinkwon Kim, Yo Han Jung, Sungwook Yu, Wook-Joo Kim, Han-Jin Cho, Kyungbok Lee, Tai Hwan Park, Mi Sun Oh, Ji Sung Lee, Joon-Tae Kim, Byung-Woo Yoon, Jong-Moo Park, Hee-Joon Bae, Keun-Hwa Jung","doi":"10.5469/neuroint.2025.00178","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>Procedure time (PT), defined as the time between groin access and vessel recanalization, is a recently recognized predictor of outcomes after endovascular thrombectomy (EVT) for acute ischemic stroke (AIS). However, the factors affecting PT and its potential value as a performance measure of AIS treatment remain unexplored.</p><p><strong>Materials and methods: </strong>Using the Korean Stroke Registry, we compared patients who underwent EVT for AIS from 2018 to 2022 based on 60 minutes PT. We conducted multivariate analysis to investigate whether PT <60 minutes was associated with successful recanalization and good functional stroke outcomes. We also investigated factors that independently predicted PT ≥60 minutes. Furthermore, we determined the cutoff point for PT.</p><p><strong>Results: </strong>We analyzed 4,703 patients (mean age: 69.5±11.9, 60.3% male) who underwent EVT. The mean PT was 54.6±36.7 minutes. Multivariate analysis revealed that PT <60 minutes independently predicted a good functional outcome as represented by modified Rankin Scale scores of 0-2 (adjusted odds ratio [aOR]: 1.40, 95% confidence interval [CI]: 1.22-1.59). PT <60 minutes was significantly associated with successful recanalization after adjusting for confounding variables (aOR: 1.66, 95% CI: 1.33-2.07). Moreover, after adjusting for covariates, age≥65 years (aOR: 1.20, 95% CI: 1.05-1.38), onset-to-door time (aOR: 1.03, 95% CI: 1.01-1.04), door-to-puncture time (aOR: 1.05, 95% CI: 1.03-1.06), posterior circulation stroke (PCS) (aOR: 1.13, 95% CI: 1.02-1.28), and smoking (aOR: 1.24, 95%CI: 1.09-1.45) independently predicted PT ≥60 minutes. Finally, the highest aOR for good stroke outcome was observed in the 60-minute cutoff model (aOR: 1.45, 95%CI: 1.27-1.67).</p><p><strong>Conclusion: </strong>PT <60 minutes was significantly associated with good functional outcomes. Conversely, PT ≥60 minutes was associated with older age, PCS, smoking, prolonged onset-to-door and door-to-puncture time. Further studies are necessary to develop refining strategies for optimizing PT to improve stroke outcomes.</p>","PeriodicalId":19140,"journal":{"name":"Neurointervention","volume":" ","pages":"71-81"},"PeriodicalIF":1.2000,"publicationDate":"2025-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12183367/pdf/","citationCount":"0","resultStr":"{\"title\":\"Procedure Time of Endovascular Thrombectomy as Performance Measure of Acute Stroke Treatment.\",\"authors\":\"Eung-Joon Lee, Han-Yeong Jeong, Jayoun Kim, Nan Hee Park, Min Kyoung Kang, Dongwhane Lee, Jinkwon Kim, Yo Han Jung, Sungwook Yu, Wook-Joo Kim, Han-Jin Cho, Kyungbok Lee, Tai Hwan Park, Mi Sun Oh, Ji Sung Lee, Joon-Tae Kim, Byung-Woo Yoon, Jong-Moo Park, Hee-Joon Bae, Keun-Hwa Jung\",\"doi\":\"10.5469/neuroint.2025.00178\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Purpose: </strong>Procedure time (PT), defined as the time between groin access and vessel recanalization, is a recently recognized predictor of outcomes after endovascular thrombectomy (EVT) for acute ischemic stroke (AIS). However, the factors affecting PT and its potential value as a performance measure of AIS treatment remain unexplored.</p><p><strong>Materials and methods: </strong>Using the Korean Stroke Registry, we compared patients who underwent EVT for AIS from 2018 to 2022 based on 60 minutes PT. We conducted multivariate analysis to investigate whether PT <60 minutes was associated with successful recanalization and good functional stroke outcomes. We also investigated factors that independently predicted PT ≥60 minutes. Furthermore, we determined the cutoff point for PT.</p><p><strong>Results: </strong>We analyzed 4,703 patients (mean age: 69.5±11.9, 60.3% male) who underwent EVT. The mean PT was 54.6±36.7 minutes. Multivariate analysis revealed that PT <60 minutes independently predicted a good functional outcome as represented by modified Rankin Scale scores of 0-2 (adjusted odds ratio [aOR]: 1.40, 95% confidence interval [CI]: 1.22-1.59). PT <60 minutes was significantly associated with successful recanalization after adjusting for confounding variables (aOR: 1.66, 95% CI: 1.33-2.07). Moreover, after adjusting for covariates, age≥65 years (aOR: 1.20, 95% CI: 1.05-1.38), onset-to-door time (aOR: 1.03, 95% CI: 1.01-1.04), door-to-puncture time (aOR: 1.05, 95% CI: 1.03-1.06), posterior circulation stroke (PCS) (aOR: 1.13, 95% CI: 1.02-1.28), and smoking (aOR: 1.24, 95%CI: 1.09-1.45) independently predicted PT ≥60 minutes. Finally, the highest aOR for good stroke outcome was observed in the 60-minute cutoff model (aOR: 1.45, 95%CI: 1.27-1.67).</p><p><strong>Conclusion: </strong>PT <60 minutes was significantly associated with good functional outcomes. Conversely, PT ≥60 minutes was associated with older age, PCS, smoking, prolonged onset-to-door and door-to-puncture time. Further studies are necessary to develop refining strategies for optimizing PT to improve stroke outcomes.</p>\",\"PeriodicalId\":19140,\"journal\":{\"name\":\"Neurointervention\",\"volume\":\" \",\"pages\":\"71-81\"},\"PeriodicalIF\":1.2000,\"publicationDate\":\"2025-07-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12183367/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Neurointervention\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.5469/neuroint.2025.00178\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/4/30 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q4\",\"JCRName\":\"CLINICAL NEUROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Neurointervention","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5469/neuroint.2025.00178","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/4/30 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
Procedure Time of Endovascular Thrombectomy as Performance Measure of Acute Stroke Treatment.
Purpose: Procedure time (PT), defined as the time between groin access and vessel recanalization, is a recently recognized predictor of outcomes after endovascular thrombectomy (EVT) for acute ischemic stroke (AIS). However, the factors affecting PT and its potential value as a performance measure of AIS treatment remain unexplored.
Materials and methods: Using the Korean Stroke Registry, we compared patients who underwent EVT for AIS from 2018 to 2022 based on 60 minutes PT. We conducted multivariate analysis to investigate whether PT <60 minutes was associated with successful recanalization and good functional stroke outcomes. We also investigated factors that independently predicted PT ≥60 minutes. Furthermore, we determined the cutoff point for PT.
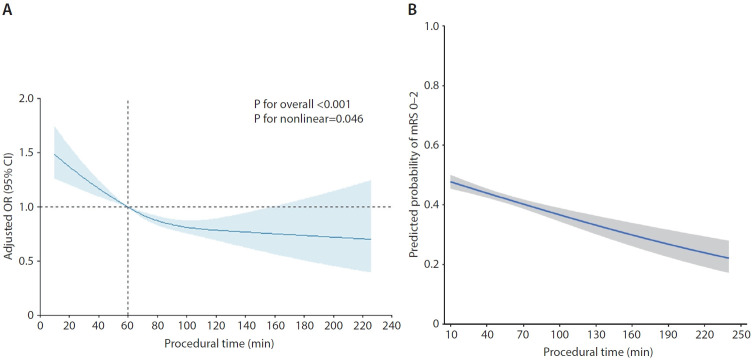
Results: We analyzed 4,703 patients (mean age: 69.5±11.9, 60.3% male) who underwent EVT. The mean PT was 54.6±36.7 minutes. Multivariate analysis revealed that PT <60 minutes independently predicted a good functional outcome as represented by modified Rankin Scale scores of 0-2 (adjusted odds ratio [aOR]: 1.40, 95% confidence interval [CI]: 1.22-1.59). PT <60 minutes was significantly associated with successful recanalization after adjusting for confounding variables (aOR: 1.66, 95% CI: 1.33-2.07). Moreover, after adjusting for covariates, age≥65 years (aOR: 1.20, 95% CI: 1.05-1.38), onset-to-door time (aOR: 1.03, 95% CI: 1.01-1.04), door-to-puncture time (aOR: 1.05, 95% CI: 1.03-1.06), posterior circulation stroke (PCS) (aOR: 1.13, 95% CI: 1.02-1.28), and smoking (aOR: 1.24, 95%CI: 1.09-1.45) independently predicted PT ≥60 minutes. Finally, the highest aOR for good stroke outcome was observed in the 60-minute cutoff model (aOR: 1.45, 95%CI: 1.27-1.67).
Conclusion: PT <60 minutes was significantly associated with good functional outcomes. Conversely, PT ≥60 minutes was associated with older age, PCS, smoking, prolonged onset-to-door and door-to-puncture time. Further studies are necessary to develop refining strategies for optimizing PT to improve stroke outcomes.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


