{"title":"因晚期围神经侵犯而行R1切除的升结肠癌加回盲切除罕见病例。","authors":"Yoshiaki Kanemoto, Tomonari Amano, Tomohiro Kurokawa, Tetsuya Tanimoto, Masahiro Amano, Kunihisa Miyazaki","doi":"10.70352/scrj.cr.25-0016","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Perineural invasion (PNI) has been cited as an independent prognostic factor in colorectal cancer. We report the first case of an additional resection after ileocecal resection due to advanced lateral extension of PNI, with a review of the literature.</p><p><strong>Case presentation: </strong>A 67-year-old woman underwent colonoscopy due to positive fecal occult blood. Biopsy revealed a 20-mm type 2 tumor in the ascending colon near the ileocecal valve, which was a poorly differentiated adenocarcinoma. She underwent laparoscopic-assisted ileocecal resection and D3 dissection, and the surgery was completed routinely in which functional end-to-end anastomosis (FEEA) was performed extracorporeally. Postoperative course was good and she was discharged one week postoperatively. The pathology showed AI, type 3, 30 × 23 mm, 40%, por2>sig>tub2, pT3a (SS), int, INFb, v2, ly3, Pn1b, PM1, DM0, pN1. There was widespread cancerous extension along the intermuscular plexus within the intrinsic muscular layer of the ileum, and although grossly separated from the tumor by about 80 mm, the tumor was R1 resected with positive oral margins. Additional anastomotic resection was performed by laparotomy. Intraoperatively, the resected section was submitted to a rapid examination, which was confirmed to be negative, and the surgery was completed. The pathological examination revealed that the resected specimen showed an adenocarcinoma on the ileum side of the anastomosis, which infiltrated and proliferated within the intermuscular plexus by about 15 mm, although the tumor was not visually recognized on the resection specimen. Both bilateral margins were negative, resulting in R0 resection. Postoperative adjuvant chemotherapy was not requested by the patient. Thereafter, periodic imaging follow-up was performed and, nine months after the initial diagnosis, there was no increase in tumor markers and no evidence of recurrence on imaging.</p><p><strong>Conclusions: </strong>Preventing R1 resection due to lateral extension of advanced PNI, which is very rare as in this case, is practically difficult given its frequency and residual bowel function. Instead, prompt additional resection and adjuvant therapy (which was not performed in this case) are essential to minimize the risk of recurrence.</p>","PeriodicalId":22096,"journal":{"name":"Surgical Case Reports","volume":"11 1","pages":""},"PeriodicalIF":0.7000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12061511/pdf/","citationCount":"0","resultStr":"{\"title\":\"Rare Case of Additional Ileocecal Resection for Ascending Colon Cancer with R1 Resection due to Advanced Perineural Invasion.\",\"authors\":\"Yoshiaki Kanemoto, Tomonari Amano, Tomohiro Kurokawa, Tetsuya Tanimoto, Masahiro Amano, Kunihisa Miyazaki\",\"doi\":\"10.70352/scrj.cr.25-0016\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Perineural invasion (PNI) has been cited as an independent prognostic factor in colorectal cancer. We report the first case of an additional resection after ileocecal resection due to advanced lateral extension of PNI, with a review of the literature.</p><p><strong>Case presentation: </strong>A 67-year-old woman underwent colonoscopy due to positive fecal occult blood. Biopsy revealed a 20-mm type 2 tumor in the ascending colon near the ileocecal valve, which was a poorly differentiated adenocarcinoma. She underwent laparoscopic-assisted ileocecal resection and D3 dissection, and the surgery was completed routinely in which functional end-to-end anastomosis (FEEA) was performed extracorporeally. Postoperative course was good and she was discharged one week postoperatively. The pathology showed AI, type 3, 30 × 23 mm, 40%, por2>sig>tub2, pT3a (SS), int, INFb, v2, ly3, Pn1b, PM1, DM0, pN1. There was widespread cancerous extension along the intermuscular plexus within the intrinsic muscular layer of the ileum, and although grossly separated from the tumor by about 80 mm, the tumor was R1 resected with positive oral margins. Additional anastomotic resection was performed by laparotomy. Intraoperatively, the resected section was submitted to a rapid examination, which was confirmed to be negative, and the surgery was completed. The pathological examination revealed that the resected specimen showed an adenocarcinoma on the ileum side of the anastomosis, which infiltrated and proliferated within the intermuscular plexus by about 15 mm, although the tumor was not visually recognized on the resection specimen. Both bilateral margins were negative, resulting in R0 resection. Postoperative adjuvant chemotherapy was not requested by the patient. Thereafter, periodic imaging follow-up was performed and, nine months after the initial diagnosis, there was no increase in tumor markers and no evidence of recurrence on imaging.</p><p><strong>Conclusions: </strong>Preventing R1 resection due to lateral extension of advanced PNI, which is very rare as in this case, is practically difficult given its frequency and residual bowel function. Instead, prompt additional resection and adjuvant therapy (which was not performed in this case) are essential to minimize the risk of recurrence.</p>\",\"PeriodicalId\":22096,\"journal\":{\"name\":\"Surgical Case Reports\",\"volume\":\"11 1\",\"pages\":\"\"},\"PeriodicalIF\":0.7000,\"publicationDate\":\"2025-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12061511/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Surgical Case Reports\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.70352/scrj.cr.25-0016\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/5/8 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q4\",\"JCRName\":\"SURGERY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Surgical Case Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.70352/scrj.cr.25-0016","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/5/8 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"SURGERY","Score":null,"Total":0}
Rare Case of Additional Ileocecal Resection for Ascending Colon Cancer with R1 Resection due to Advanced Perineural Invasion.
Introduction: Perineural invasion (PNI) has been cited as an independent prognostic factor in colorectal cancer. We report the first case of an additional resection after ileocecal resection due to advanced lateral extension of PNI, with a review of the literature.
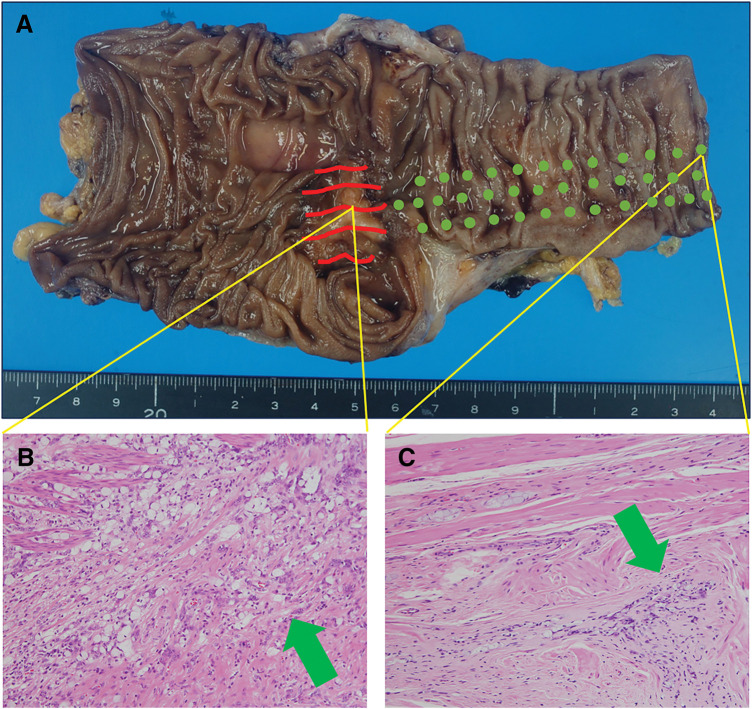
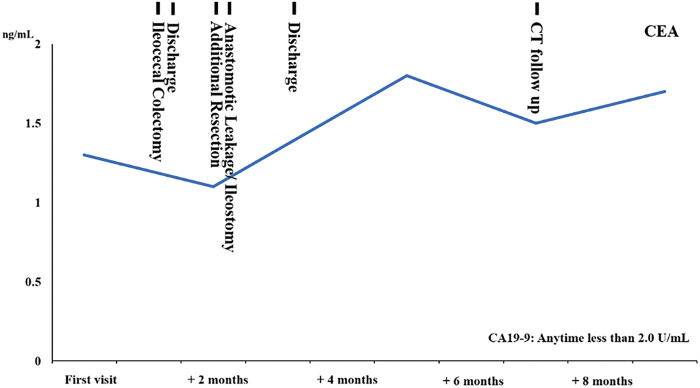
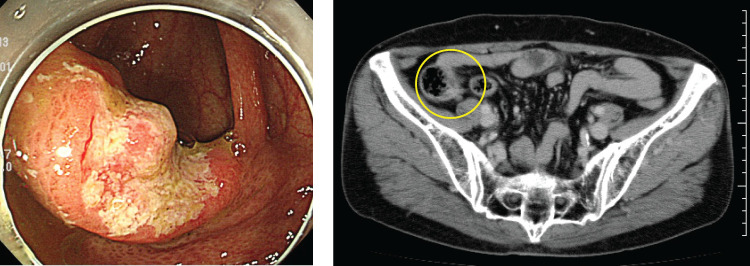
Case presentation: A 67-year-old woman underwent colonoscopy due to positive fecal occult blood. Biopsy revealed a 20-mm type 2 tumor in the ascending colon near the ileocecal valve, which was a poorly differentiated adenocarcinoma. She underwent laparoscopic-assisted ileocecal resection and D3 dissection, and the surgery was completed routinely in which functional end-to-end anastomosis (FEEA) was performed extracorporeally. Postoperative course was good and she was discharged one week postoperatively. The pathology showed AI, type 3, 30 × 23 mm, 40%, por2>sig>tub2, pT3a (SS), int, INFb, v2, ly3, Pn1b, PM1, DM0, pN1. There was widespread cancerous extension along the intermuscular plexus within the intrinsic muscular layer of the ileum, and although grossly separated from the tumor by about 80 mm, the tumor was R1 resected with positive oral margins. Additional anastomotic resection was performed by laparotomy. Intraoperatively, the resected section was submitted to a rapid examination, which was confirmed to be negative, and the surgery was completed. The pathological examination revealed that the resected specimen showed an adenocarcinoma on the ileum side of the anastomosis, which infiltrated and proliferated within the intermuscular plexus by about 15 mm, although the tumor was not visually recognized on the resection specimen. Both bilateral margins were negative, resulting in R0 resection. Postoperative adjuvant chemotherapy was not requested by the patient. Thereafter, periodic imaging follow-up was performed and, nine months after the initial diagnosis, there was no increase in tumor markers and no evidence of recurrence on imaging.
Conclusions: Preventing R1 resection due to lateral extension of advanced PNI, which is very rare as in this case, is practically difficult given its frequency and residual bowel function. Instead, prompt additional resection and adjuvant therapy (which was not performed in this case) are essential to minimize the risk of recurrence.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


