R Sguinzi, J Fiechter, L Bafumi, B Gremaud, B Geng, P Janiak, L Bühler, B Egger
{"title":"保留括约肌的直肠癌手术后出现低位前切除术综合征患者的评分评估与治疗。","authors":"R Sguinzi, J Fiechter, L Bafumi, B Gremaud, B Geng, P Janiak, L Bühler, B Egger","doi":"10.1007/s00384-025-04906-w","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Sphincter-sparing low anterior resection (SSLAR) with neoadjuvant radio-chemotherapy has been developed to avoid abdomino-perineal amputation and permanent colostomy in patients with low rectal cancer. However, many patients develop symptoms known as low anterior resection syndrome (LARS), including fecal urgency, incontinence, and a sensation of incomplete evacuation. The Low Anterior Resection Syndrome Score (LARS Score), a validated tool developed by Emmertsen and Laurberg, is used to assess symptom severity and guide treatment.</p><p><strong>Materials and methods: </strong>We present a single-center cohort study including patients having undergone SSLAR for rectal cancer between 2014 and 2021 at Fribourg Cantonal Hospital. Initial LARS-scores were obtained by completion of the QoL questionnaire. Patients with minor LARS (scores 21-29) were treated with electrostimulation and bio-feedback physiotherapy. Those with major LARS (scores > 29) were first investigated by anal manometry followed by physiotherapy. All treatments took place in 2022/2023. After treatment, LARS-scores were calculated again.</p><p><strong>Results: </strong>Of 54 patients included in the study, 18.5% had minor LARS, 40.8% major LARS, and 40.8% had no LARS. Of all patients with LARS, 18 (56%) completed pelvic physiotherapy, whereas 14 (44%) refused the treatment. Before and after pelvic physiotherapy, the median LARS score was 32 [interquartile range 29.50-38.50] and 22.5 [18.5-28], respectively (p < 0.001 according to Wilcoxon signed-rank test). Analysis of risk factors did not reveal any significant difference in age, gender, diabetes, nicotine or alcohol use, previous abdominal surgery, tumor stage, chemo/radiotherapy, type of operation and anastomosis, or anastomotic leakage.</p><p><strong>Conclusions: </strong>Approximately half of patients undergoing SSLAR experience LARS, and approximately one-third develop the major form. LARS scores may significantly improve with specific physiotherapeutic measures that have therefore been introduced as a standard procedure for all SSLAR patients at our institution.</p>","PeriodicalId":13789,"journal":{"name":"International Journal of Colorectal Disease","volume":"40 1","pages":"115"},"PeriodicalIF":2.3000,"publicationDate":"2025-05-14","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12078403/pdf/","citationCount":"0","resultStr":"{\"title\":\"Score assessment and treatment in patients presenting with low anterior resection syndrome after sphincter-sparing rectal cancer surgery.\",\"authors\":\"R Sguinzi, J Fiechter, L Bafumi, B Gremaud, B Geng, P Janiak, L Bühler, B Egger\",\"doi\":\"10.1007/s00384-025-04906-w\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Sphincter-sparing low anterior resection (SSLAR) with neoadjuvant radio-chemotherapy has been developed to avoid abdomino-perineal amputation and permanent colostomy in patients with low rectal cancer. However, many patients develop symptoms known as low anterior resection syndrome (LARS), including fecal urgency, incontinence, and a sensation of incomplete evacuation. The Low Anterior Resection Syndrome Score (LARS Score), a validated tool developed by Emmertsen and Laurberg, is used to assess symptom severity and guide treatment.</p><p><strong>Materials and methods: </strong>We present a single-center cohort study including patients having undergone SSLAR for rectal cancer between 2014 and 2021 at Fribourg Cantonal Hospital. Initial LARS-scores were obtained by completion of the QoL questionnaire. Patients with minor LARS (scores 21-29) were treated with electrostimulation and bio-feedback physiotherapy. Those with major LARS (scores > 29) were first investigated by anal manometry followed by physiotherapy. All treatments took place in 2022/2023. After treatment, LARS-scores were calculated again.</p><p><strong>Results: </strong>Of 54 patients included in the study, 18.5% had minor LARS, 40.8% major LARS, and 40.8% had no LARS. Of all patients with LARS, 18 (56%) completed pelvic physiotherapy, whereas 14 (44%) refused the treatment. Before and after pelvic physiotherapy, the median LARS score was 32 [interquartile range 29.50-38.50] and 22.5 [18.5-28], respectively (p < 0.001 according to Wilcoxon signed-rank test). Analysis of risk factors did not reveal any significant difference in age, gender, diabetes, nicotine or alcohol use, previous abdominal surgery, tumor stage, chemo/radiotherapy, type of operation and anastomosis, or anastomotic leakage.</p><p><strong>Conclusions: </strong>Approximately half of patients undergoing SSLAR experience LARS, and approximately one-third develop the major form. LARS scores may significantly improve with specific physiotherapeutic measures that have therefore been introduced as a standard procedure for all SSLAR patients at our institution.</p>\",\"PeriodicalId\":13789,\"journal\":{\"name\":\"International Journal of Colorectal Disease\",\"volume\":\"40 1\",\"pages\":\"115\"},\"PeriodicalIF\":2.3000,\"publicationDate\":\"2025-05-14\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12078403/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"International Journal of Colorectal Disease\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s00384-025-04906-w\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"International Journal of Colorectal Disease","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s00384-025-04906-w","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
Score assessment and treatment in patients presenting with low anterior resection syndrome after sphincter-sparing rectal cancer surgery.
Background: Sphincter-sparing low anterior resection (SSLAR) with neoadjuvant radio-chemotherapy has been developed to avoid abdomino-perineal amputation and permanent colostomy in patients with low rectal cancer. However, many patients develop symptoms known as low anterior resection syndrome (LARS), including fecal urgency, incontinence, and a sensation of incomplete evacuation. The Low Anterior Resection Syndrome Score (LARS Score), a validated tool developed by Emmertsen and Laurberg, is used to assess symptom severity and guide treatment.
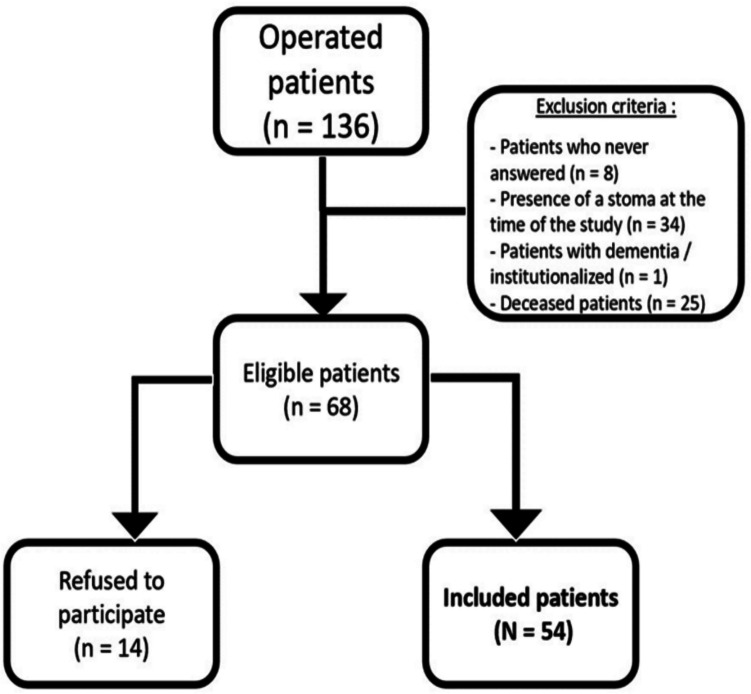
Materials and methods: We present a single-center cohort study including patients having undergone SSLAR for rectal cancer between 2014 and 2021 at Fribourg Cantonal Hospital. Initial LARS-scores were obtained by completion of the QoL questionnaire. Patients with minor LARS (scores 21-29) were treated with electrostimulation and bio-feedback physiotherapy. Those with major LARS (scores > 29) were first investigated by anal manometry followed by physiotherapy. All treatments took place in 2022/2023. After treatment, LARS-scores were calculated again.
Results: Of 54 patients included in the study, 18.5% had minor LARS, 40.8% major LARS, and 40.8% had no LARS. Of all patients with LARS, 18 (56%) completed pelvic physiotherapy, whereas 14 (44%) refused the treatment. Before and after pelvic physiotherapy, the median LARS score was 32 [interquartile range 29.50-38.50] and 22.5 [18.5-28], respectively (p < 0.001 according to Wilcoxon signed-rank test). Analysis of risk factors did not reveal any significant difference in age, gender, diabetes, nicotine or alcohol use, previous abdominal surgery, tumor stage, chemo/radiotherapy, type of operation and anastomosis, or anastomotic leakage.
Conclusions: Approximately half of patients undergoing SSLAR experience LARS, and approximately one-third develop the major form. LARS scores may significantly improve with specific physiotherapeutic measures that have therefore been introduced as a standard procedure for all SSLAR patients at our institution.
期刊介绍:
The International Journal of Colorectal Disease, Clinical and Molecular Gastroenterology and Surgery aims to publish novel and state-of-the-art papers which deal with the physiology and pathophysiology of diseases involving the entire gastrointestinal tract. In addition to original research articles, the following categories will be included: reviews (usually commissioned but may also be submitted), case reports, letters to the editor, and protocols on clinical studies.
The journal offers its readers an interdisciplinary forum for clinical science and molecular research related to gastrointestinal disease.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


