{"title":"BUN/肌酐比值在判断消化道出血严重程度及出血定位中的作用。","authors":"Aslihan Calim","doi":"10.14744/nci.2025.34366","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>The aim of the study is to evaluate an established biomarker such as blood urea nitrogen (BUN)/Creatinine ratio in predicting upper gastrointestinal bleeding versus lower GI and stratify its severity. The aim of this study is to evaluate the diagnostic performance in clinical practice and predestination as a prognostic factor, including admission to an intensive care unit (ICU) or mortality rate for BUN/Creatinine ratio.</p><p><strong>Methods: </strong>A total of 300 patients controlled in our hospital between January 2022 and January 2024 were evaluated retrospectively due to hospitalization by acute GI bleeding. Gastroscopy and/or colonoscopy were used to stratify patients into the upper or lower GI bleeding group. Data included demographic information, clinical presentation history and vital signs, comorbidity status, medication use, clinical outcomes and laboratory tests including hemoglobin, hematocrit, urea, creatinine levels and so on. The BUN/Creatinine ratio was determined and correlated with site as well as severity of bleeding. Statistical techniques, such as logistic regression and receiver operating characteristic (ROC) analysis, were used to assess the diagnostic performance of the ratio and to choose a cut-off value.</p><p><strong>Results: </strong>Among the 300 patients, 215 (71.7% had upper GI bleeding, and 85 (28.3% had lower GI bleeding. Hematemesis and melena were significantly associated with upper GI bleeding, whereas hematochezia was more common in lower GI bleeding. Patients with upper GI bleeding had significantly higher BUN, urea, and BUN/Creatinine ratios, while hemoglobin and hematocrit levels were lower. The optimal BUN/Creatinine cut-off value of 23.3 demonstrated high sensitivity (89.3%) and specificity (94.1%) for distinguishing between upper and lower GI bleeding. Multivariate analysis revealed BUN/Creatinine ratio, hematochezia and endoscopic intervention as an independent predictor of bleeding location. Patients with BUN/Creatinine ratio >23.3 showed increased frequency of red blood cell transfusion, endoscopic intervention, and mortality.</p><p><strong>Conclusion: </strong>The BUN/Creatinine ratio is a sensitive, noninvasive biomarker for distinguishing between upper and lower GI bleed and severity. Its introduction into clinical practice may enhance the decision process and patient care, especially in critical care contexts. Additional research is indicated to confirm these results and to define standardized cut-off values for wider use.</p>","PeriodicalId":94347,"journal":{"name":"Northern clinics of Istanbul","volume":"12 2","pages":"244-252"},"PeriodicalIF":0.9000,"publicationDate":"2025-04-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12051006/pdf/","citationCount":"0","resultStr":"{\"title\":\"The role of BUN/creatinine ratio in determining the severity of gastrointestinal bleeding and bleeding localization.\",\"authors\":\"Aslihan Calim\",\"doi\":\"10.14744/nci.2025.34366\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>The aim of the study is to evaluate an established biomarker such as blood urea nitrogen (BUN)/Creatinine ratio in predicting upper gastrointestinal bleeding versus lower GI and stratify its severity. The aim of this study is to evaluate the diagnostic performance in clinical practice and predestination as a prognostic factor, including admission to an intensive care unit (ICU) or mortality rate for BUN/Creatinine ratio.</p><p><strong>Methods: </strong>A total of 300 patients controlled in our hospital between January 2022 and January 2024 were evaluated retrospectively due to hospitalization by acute GI bleeding. Gastroscopy and/or colonoscopy were used to stratify patients into the upper or lower GI bleeding group. Data included demographic information, clinical presentation history and vital signs, comorbidity status, medication use, clinical outcomes and laboratory tests including hemoglobin, hematocrit, urea, creatinine levels and so on. The BUN/Creatinine ratio was determined and correlated with site as well as severity of bleeding. Statistical techniques, such as logistic regression and receiver operating characteristic (ROC) analysis, were used to assess the diagnostic performance of the ratio and to choose a cut-off value.</p><p><strong>Results: </strong>Among the 300 patients, 215 (71.7% had upper GI bleeding, and 85 (28.3% had lower GI bleeding. Hematemesis and melena were significantly associated with upper GI bleeding, whereas hematochezia was more common in lower GI bleeding. Patients with upper GI bleeding had significantly higher BUN, urea, and BUN/Creatinine ratios, while hemoglobin and hematocrit levels were lower. The optimal BUN/Creatinine cut-off value of 23.3 demonstrated high sensitivity (89.3%) and specificity (94.1%) for distinguishing between upper and lower GI bleeding. Multivariate analysis revealed BUN/Creatinine ratio, hematochezia and endoscopic intervention as an independent predictor of bleeding location. Patients with BUN/Creatinine ratio >23.3 showed increased frequency of red blood cell transfusion, endoscopic intervention, and mortality.</p><p><strong>Conclusion: </strong>The BUN/Creatinine ratio is a sensitive, noninvasive biomarker for distinguishing between upper and lower GI bleed and severity. Its introduction into clinical practice may enhance the decision process and patient care, especially in critical care contexts. Additional research is indicated to confirm these results and to define standardized cut-off values for wider use.</p>\",\"PeriodicalId\":94347,\"journal\":{\"name\":\"Northern clinics of Istanbul\",\"volume\":\"12 2\",\"pages\":\"244-252\"},\"PeriodicalIF\":0.9000,\"publicationDate\":\"2025-04-28\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12051006/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Northern clinics of Istanbul\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.14744/nci.2025.34366\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Northern clinics of Istanbul","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.14744/nci.2025.34366","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
The role of BUN/creatinine ratio in determining the severity of gastrointestinal bleeding and bleeding localization.
Objective: The aim of the study is to evaluate an established biomarker such as blood urea nitrogen (BUN)/Creatinine ratio in predicting upper gastrointestinal bleeding versus lower GI and stratify its severity. The aim of this study is to evaluate the diagnostic performance in clinical practice and predestination as a prognostic factor, including admission to an intensive care unit (ICU) or mortality rate for BUN/Creatinine ratio.
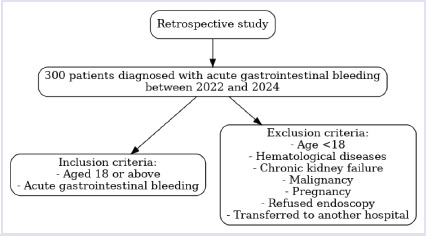
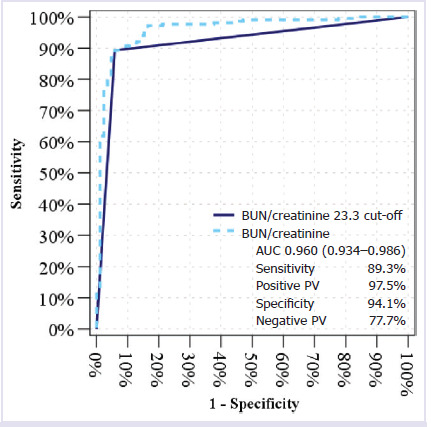
Methods: A total of 300 patients controlled in our hospital between January 2022 and January 2024 were evaluated retrospectively due to hospitalization by acute GI bleeding. Gastroscopy and/or colonoscopy were used to stratify patients into the upper or lower GI bleeding group. Data included demographic information, clinical presentation history and vital signs, comorbidity status, medication use, clinical outcomes and laboratory tests including hemoglobin, hematocrit, urea, creatinine levels and so on. The BUN/Creatinine ratio was determined and correlated with site as well as severity of bleeding. Statistical techniques, such as logistic regression and receiver operating characteristic (ROC) analysis, were used to assess the diagnostic performance of the ratio and to choose a cut-off value.
Results: Among the 300 patients, 215 (71.7% had upper GI bleeding, and 85 (28.3% had lower GI bleeding. Hematemesis and melena were significantly associated with upper GI bleeding, whereas hematochezia was more common in lower GI bleeding. Patients with upper GI bleeding had significantly higher BUN, urea, and BUN/Creatinine ratios, while hemoglobin and hematocrit levels were lower. The optimal BUN/Creatinine cut-off value of 23.3 demonstrated high sensitivity (89.3%) and specificity (94.1%) for distinguishing between upper and lower GI bleeding. Multivariate analysis revealed BUN/Creatinine ratio, hematochezia and endoscopic intervention as an independent predictor of bleeding location. Patients with BUN/Creatinine ratio >23.3 showed increased frequency of red blood cell transfusion, endoscopic intervention, and mortality.
Conclusion: The BUN/Creatinine ratio is a sensitive, noninvasive biomarker for distinguishing between upper and lower GI bleed and severity. Its introduction into clinical practice may enhance the decision process and patient care, especially in critical care contexts. Additional research is indicated to confirm these results and to define standardized cut-off values for wider use.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


