Yash Akkara, Joshua J Hon, Mahathir Ahmed, Basel Musmar, Joanna Roy, Stavropoula Tjoumakaris, Michael Reid Gooch, Robert H Rosenwasser, Pascal Jabbour
{"title":"颈动脉内膜切除术与颈动脉支架置入的成本-效果:系统回顾和荟萃分析。","authors":"Yash Akkara, Joshua J Hon, Mahathir Ahmed, Basel Musmar, Joanna Roy, Stavropoula Tjoumakaris, Michael Reid Gooch, Robert H Rosenwasser, Pascal Jabbour","doi":"10.1007/s12975-025-01347-z","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Carotid artery stenting (CAS) and carotid endarterectomy (CEA) are gold-standard treatments of carotid artery stenosis. This study aims to identify the cost-effectiveness of CEA vs CAS.</p><p><strong>Methods: </strong>Studies were screened through PubMed, MEDLINE, and Embase using PRISMA guidelines, and required ≥ 20 participants who were ≥ 16 years, alongside costs at 1-year postoperatively. The Shapiro-Wilk test, independent sample t-tests, ANOVA, and Spearman's R were used, with costs adjusted to 2024. A random-effects model was used to compare cost-effectiveness. Bias assessment was according to the Cochrane Risk of Bias 2.0 tool and the Newcastle-Ottawa Scale.</p><p><strong>Results: </strong>7 studies were included, with a sample of 6493 participants (3418 M, 3075 F). 2932 and 3511 participants underwent CEA and CAS respectively. CEA reported a significantly longer mean length of procedure (191.92 vs. 77.5 min, p < 0.0001) and length of stay (3.13 vs. 2.60 days, p < 0.0001) vs. CAS. The mean adjusted cost of CEA and CAS were $18156.60 (6466) and $17711.01 (5511) respectively. Studies reported lower risks of stroke (2.12% vs. 3.65%, p < 0.001), higher risks of myocardial infarctions (1.70% vs. 1.42%, p < 0.01), and higher risks of other complications for CEA vs. CAS respectively. The expected 1-year cost of CEA was marginally lower than CAS ($21264.03 vs. $21433.14, p < 0.05). The cost-effectiveness of CEA was marginally better than CAS (ratio = 1.019, 95% CI [1.017, 1.020)].</p><p><strong>Conclusions: </strong>CEA provides marginally improved cost-effectiveness over CAS, providing long-term cost benefits to centers with large surgical volumes. However, shorter procedural times and inpatient stays with CAS may improve overall productivity. Cost should hence not be a deciding factor when choosing between CEA and CAS.</p>","PeriodicalId":23237,"journal":{"name":"Translational Stroke Research","volume":" ","pages":"1874-1883"},"PeriodicalIF":4.3000,"publicationDate":"2025-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12391230/pdf/","citationCount":"0","resultStr":"{\"title\":\"Cost-Effectiveness of Carotid Endarterectomy vs. Carotid Stenting: a Systematic Review and Meta-Analysis.\",\"authors\":\"Yash Akkara, Joshua J Hon, Mahathir Ahmed, Basel Musmar, Joanna Roy, Stavropoula Tjoumakaris, Michael Reid Gooch, Robert H Rosenwasser, Pascal Jabbour\",\"doi\":\"10.1007/s12975-025-01347-z\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Carotid artery stenting (CAS) and carotid endarterectomy (CEA) are gold-standard treatments of carotid artery stenosis. This study aims to identify the cost-effectiveness of CEA vs CAS.</p><p><strong>Methods: </strong>Studies were screened through PubMed, MEDLINE, and Embase using PRISMA guidelines, and required ≥ 20 participants who were ≥ 16 years, alongside costs at 1-year postoperatively. The Shapiro-Wilk test, independent sample t-tests, ANOVA, and Spearman's R were used, with costs adjusted to 2024. A random-effects model was used to compare cost-effectiveness. Bias assessment was according to the Cochrane Risk of Bias 2.0 tool and the Newcastle-Ottawa Scale.</p><p><strong>Results: </strong>7 studies were included, with a sample of 6493 participants (3418 M, 3075 F). 2932 and 3511 participants underwent CEA and CAS respectively. CEA reported a significantly longer mean length of procedure (191.92 vs. 77.5 min, p < 0.0001) and length of stay (3.13 vs. 2.60 days, p < 0.0001) vs. CAS. The mean adjusted cost of CEA and CAS were $18156.60 (6466) and $17711.01 (5511) respectively. Studies reported lower risks of stroke (2.12% vs. 3.65%, p < 0.001), higher risks of myocardial infarctions (1.70% vs. 1.42%, p < 0.01), and higher risks of other complications for CEA vs. CAS respectively. The expected 1-year cost of CEA was marginally lower than CAS ($21264.03 vs. $21433.14, p < 0.05). The cost-effectiveness of CEA was marginally better than CAS (ratio = 1.019, 95% CI [1.017, 1.020)].</p><p><strong>Conclusions: </strong>CEA provides marginally improved cost-effectiveness over CAS, providing long-term cost benefits to centers with large surgical volumes. However, shorter procedural times and inpatient stays with CAS may improve overall productivity. Cost should hence not be a deciding factor when choosing between CEA and CAS.</p>\",\"PeriodicalId\":23237,\"journal\":{\"name\":\"Translational Stroke Research\",\"volume\":\" \",\"pages\":\"1874-1883\"},\"PeriodicalIF\":4.3000,\"publicationDate\":\"2025-10-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12391230/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Translational Stroke Research\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s12975-025-01347-z\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/4/11 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q1\",\"JCRName\":\"CLINICAL NEUROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Translational Stroke Research","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s12975-025-01347-z","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/4/11 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
摘要
颈动脉支架植入术(CAS)和颈动脉内膜切除术(CEA)是治疗颈动脉狭窄的金标准。本研究旨在确定CEA与CAS的成本效益。方法:使用PRISMA指南通过PubMed、MEDLINE和Embase筛选研究,并要求≥20名年龄≥16岁的参与者,以及术后1年的成本。采用夏皮罗-威尔克检验、独立样本t检验、方差分析和斯皮尔曼R,成本调整为2024。采用随机效应模型比较成本-效果。偏倚评估依据Cochrane Risk of Bias 2.0工具和Newcastle-Ottawa量表。结果:纳入7项研究,共纳入6493例受试者(男3418例,女3075例),其中CEA和CAS分别为2932例和3511例。CEA报告的平均手术时间明显更长(191.92分钟vs 77.5分钟),结论:CEA比CAS略微提高了成本效益,为大手术量的中心提供了长期的成本效益。然而,更短的手术时间和住院时间可以提高CAS的整体生产力。因此,在CEA和CAS之间进行选择时,成本不应成为决定因素。
Cost-Effectiveness of Carotid Endarterectomy vs. Carotid Stenting: a Systematic Review and Meta-Analysis.
Introduction: Carotid artery stenting (CAS) and carotid endarterectomy (CEA) are gold-standard treatments of carotid artery stenosis. This study aims to identify the cost-effectiveness of CEA vs CAS.
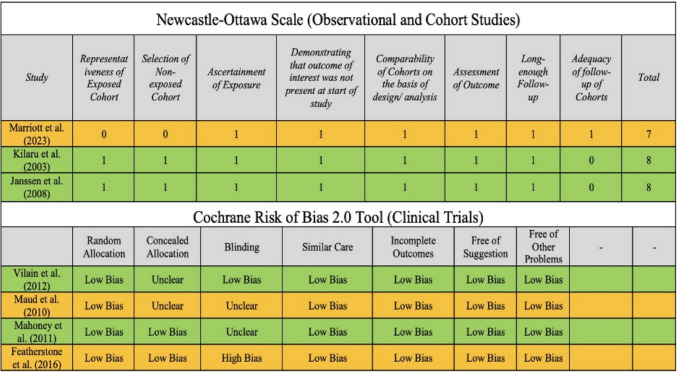
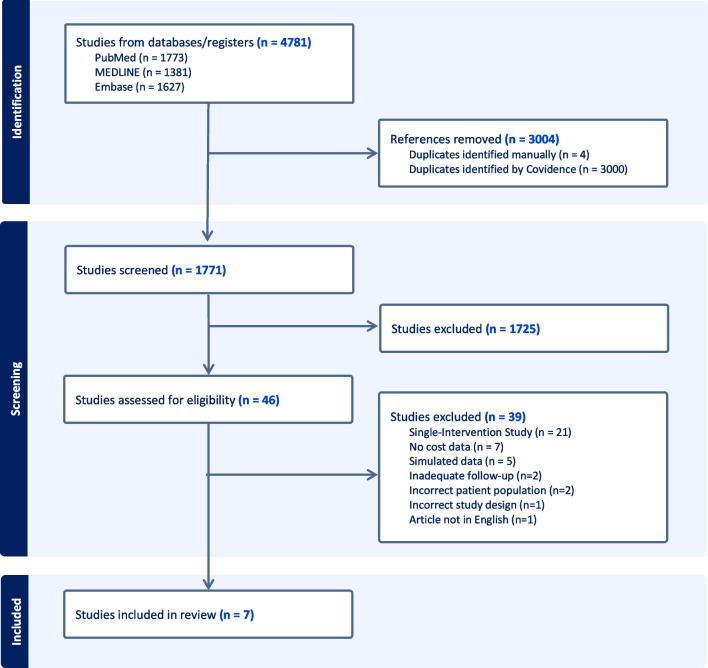
Methods: Studies were screened through PubMed, MEDLINE, and Embase using PRISMA guidelines, and required ≥ 20 participants who were ≥ 16 years, alongside costs at 1-year postoperatively. The Shapiro-Wilk test, independent sample t-tests, ANOVA, and Spearman's R were used, with costs adjusted to 2024. A random-effects model was used to compare cost-effectiveness. Bias assessment was according to the Cochrane Risk of Bias 2.0 tool and the Newcastle-Ottawa Scale.
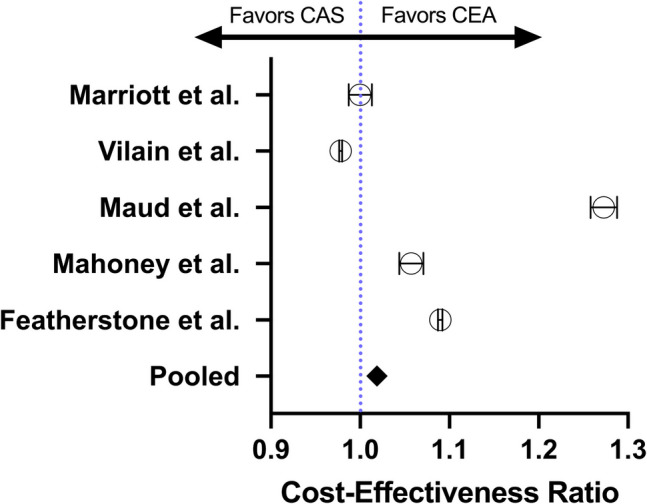
Results: 7 studies were included, with a sample of 6493 participants (3418 M, 3075 F). 2932 and 3511 participants underwent CEA and CAS respectively. CEA reported a significantly longer mean length of procedure (191.92 vs. 77.5 min, p < 0.0001) and length of stay (3.13 vs. 2.60 days, p < 0.0001) vs. CAS. The mean adjusted cost of CEA and CAS were $18156.60 (6466) and $17711.01 (5511) respectively. Studies reported lower risks of stroke (2.12% vs. 3.65%, p < 0.001), higher risks of myocardial infarctions (1.70% vs. 1.42%, p < 0.01), and higher risks of other complications for CEA vs. CAS respectively. The expected 1-year cost of CEA was marginally lower than CAS ($21264.03 vs. $21433.14, p < 0.05). The cost-effectiveness of CEA was marginally better than CAS (ratio = 1.019, 95% CI [1.017, 1.020)].
Conclusions: CEA provides marginally improved cost-effectiveness over CAS, providing long-term cost benefits to centers with large surgical volumes. However, shorter procedural times and inpatient stays with CAS may improve overall productivity. Cost should hence not be a deciding factor when choosing between CEA and CAS.
期刊介绍:
Translational Stroke Research covers basic, translational, and clinical studies. The Journal emphasizes novel approaches to help both to understand clinical phenomenon through basic science tools, and to translate basic science discoveries into the development of new strategies for the prevention, assessment, treatment, and enhancement of central nervous system repair after stroke and other forms of neurotrauma.
Translational Stroke Research focuses on translational research and is relevant to both basic scientists and physicians, including but not restricted to neuroscientists, vascular biologists, neurologists, neuroimagers, and neurosurgeons.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


