Mahmoud Al-Masri, Yasmin Safi, Osama Alayyan, Ramiz Kardan, Laith Al Khraisat, Ahmad Massad, Farah Alsadi
{"title":"新型冠状病毒感染后癌症患者择期手术时机优化大流行后分析。","authors":"Mahmoud Al-Masri, Yasmin Safi, Osama Alayyan, Ramiz Kardan, Laith Al Khraisat, Ahmad Massad, Farah Alsadi","doi":"10.1186/s13027-025-00646-2","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>The COVID-19 pandemic introduced challenges including delaying elective surgery. For cancer patients, reducing delays is preferred to prevent unfavorable outcomes. there is a lack of consensus regarding the optimal timing of elective surgery following a SARS-CoV-2. This study aimed to find the optimal time to elective surgery to minimize 30-day postoperative morbidity and mortality.</p><p><strong>Methods: </strong>This is a retrospective chart review of all adult patients who underwent elective surgery with a confirmed preoperative COVID-19 diagnosis between September 2020 and April 2023. Patients' elective surgeries delays were examined to determine the optimal time to surgery in terms of postoperative complications. Analysis was controlled for age, ASA score, comorbidities, and smoking status.</p><p><strong>Results: </strong>358 records examined, 94.7% had delayed surgery and 5.3% had cancelled surgery. The optimal time to surgery was ≥ 17 days to minimize postoperative pulmonary complications [OR: 0.299, p = 0.048], other postoperative complications [OR: 0.459, p = 0.01], and a decrease in length of hospital stay. In multivariate analysis, the only significant predictors for postoperative complications were time to surgery; surgery ≥ 17 days after diagnosis had better postoperative outcomes [p < 0.001], and COVID-19 symptoms status [p = 0.019].</p><p><strong>Conclusion: </strong>The best time to surgery in this cohort is at least 17 days (or a range of 2-3 weeks) for optimal results. Further research is needed to investigate the effect of such delays on oncological outcomes in this cohort.</p>","PeriodicalId":13568,"journal":{"name":"Infectious Agents and Cancer","volume":"20 1","pages":"25"},"PeriodicalIF":2.8000,"publicationDate":"2025-04-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11998221/pdf/","citationCount":"0","resultStr":"{\"title\":\"Optimizing timing for elective surgery in cancer patients following COVID-19 infection; a post-pandemic analysis.\",\"authors\":\"Mahmoud Al-Masri, Yasmin Safi, Osama Alayyan, Ramiz Kardan, Laith Al Khraisat, Ahmad Massad, Farah Alsadi\",\"doi\":\"10.1186/s13027-025-00646-2\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>The COVID-19 pandemic introduced challenges including delaying elective surgery. For cancer patients, reducing delays is preferred to prevent unfavorable outcomes. there is a lack of consensus regarding the optimal timing of elective surgery following a SARS-CoV-2. This study aimed to find the optimal time to elective surgery to minimize 30-day postoperative morbidity and mortality.</p><p><strong>Methods: </strong>This is a retrospective chart review of all adult patients who underwent elective surgery with a confirmed preoperative COVID-19 diagnosis between September 2020 and April 2023. Patients' elective surgeries delays were examined to determine the optimal time to surgery in terms of postoperative complications. Analysis was controlled for age, ASA score, comorbidities, and smoking status.</p><p><strong>Results: </strong>358 records examined, 94.7% had delayed surgery and 5.3% had cancelled surgery. The optimal time to surgery was ≥ 17 days to minimize postoperative pulmonary complications [OR: 0.299, p = 0.048], other postoperative complications [OR: 0.459, p = 0.01], and a decrease in length of hospital stay. In multivariate analysis, the only significant predictors for postoperative complications were time to surgery; surgery ≥ 17 days after diagnosis had better postoperative outcomes [p < 0.001], and COVID-19 symptoms status [p = 0.019].</p><p><strong>Conclusion: </strong>The best time to surgery in this cohort is at least 17 days (or a range of 2-3 weeks) for optimal results. Further research is needed to investigate the effect of such delays on oncological outcomes in this cohort.</p>\",\"PeriodicalId\":13568,\"journal\":{\"name\":\"Infectious Agents and Cancer\",\"volume\":\"20 1\",\"pages\":\"25\"},\"PeriodicalIF\":2.8000,\"publicationDate\":\"2025-04-15\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11998221/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Infectious Agents and Cancer\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1186/s13027-025-00646-2\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"IMMUNOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Infectious Agents and Cancer","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s13027-025-00646-2","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"IMMUNOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
新冠肺炎大流行带来的挑战包括推迟择期手术。对于癌症患者来说,减少延迟是预防不良后果的首选。关于SARS-CoV-2后择期手术的最佳时机缺乏共识。本研究旨在寻找择期手术的最佳时间,以尽量减少术后30天的发病率和死亡率。方法:对2020年9月至2023年4月期间术前确诊COVID-19并接受择期手术的所有成年患者进行回顾性图表回顾。检查患者的选择性手术延迟,以确定手术的最佳时间在术后并发症方面。分析控制年龄、ASA评分、合并症和吸烟状况。结果:检查病历358例,延迟手术94.7%,取消手术5.3%。最佳手术时间≥17天,以减少术后肺部并发症[OR: 0.299, p = 0.048]和其他术后并发症[OR: 0.459, p = 0.01],并减少住院时间。在多变量分析中,术后并发症的唯一显著预测因素是手术时间;结论:该队列中最佳手术时间至少为17天(或2-3周范围),以获得最佳效果。需要进一步的研究来调查这种延迟对该队列肿瘤预后的影响。
Optimizing timing for elective surgery in cancer patients following COVID-19 infection; a post-pandemic analysis.
Introduction: The COVID-19 pandemic introduced challenges including delaying elective surgery. For cancer patients, reducing delays is preferred to prevent unfavorable outcomes. there is a lack of consensus regarding the optimal timing of elective surgery following a SARS-CoV-2. This study aimed to find the optimal time to elective surgery to minimize 30-day postoperative morbidity and mortality.
Methods: This is a retrospective chart review of all adult patients who underwent elective surgery with a confirmed preoperative COVID-19 diagnosis between September 2020 and April 2023. Patients' elective surgeries delays were examined to determine the optimal time to surgery in terms of postoperative complications. Analysis was controlled for age, ASA score, comorbidities, and smoking status.
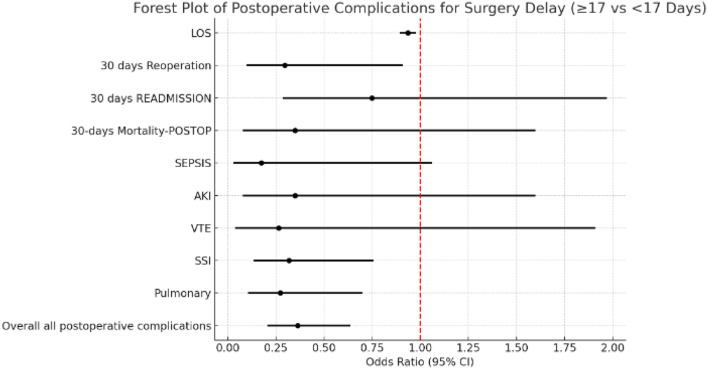
Results: 358 records examined, 94.7% had delayed surgery and 5.3% had cancelled surgery. The optimal time to surgery was ≥ 17 days to minimize postoperative pulmonary complications [OR: 0.299, p = 0.048], other postoperative complications [OR: 0.459, p = 0.01], and a decrease in length of hospital stay. In multivariate analysis, the only significant predictors for postoperative complications were time to surgery; surgery ≥ 17 days after diagnosis had better postoperative outcomes [p < 0.001], and COVID-19 symptoms status [p = 0.019].
Conclusion: The best time to surgery in this cohort is at least 17 days (or a range of 2-3 weeks) for optimal results. Further research is needed to investigate the effect of such delays on oncological outcomes in this cohort.
期刊介绍:
Infectious Agents and Cancer is an open access, peer-reviewed online journal that encompasses all aspects of basic, clinical, epidemiological and translational research providing an insight into the association between chronic infections and cancer.
The journal welcomes submissions in the pathogen-related cancer areas and other related topics, in particular:
• HPV and anogenital cancers, as well as head and neck cancers;
• EBV and Burkitt lymphoma;
• HCV/HBV and hepatocellular carcinoma as well as lymphoproliferative diseases;
• HHV8 and Kaposi sarcoma;
• HTLV and leukemia;
• Cancers in Low- and Middle-income countries.
The link between infection and cancer has become well established over the past 50 years, and infection-associated cancer contribute up to 16% of cancers in developed countries and 33% in less developed countries.
Preventive vaccines have been developed for only two cancer-causing viruses, highlighting both the opportunity to prevent infection-associated cancers by vaccination and the gaps that remain before vaccines can be developed for other cancer-causing agents. These gaps are due to incomplete understanding of the basic biology, natural history, epidemiology of many of the pathogens that cause cancer, the mechanisms they exploit to cause cancer, and how to interrupt progression to cancer in human populations. Early diagnosis or identification of lesions at high risk of progression represent the current most critical research area of the field supported by recent advances in genomics and proteomics technologies.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


