Nathaniel E Zona, Michael A Hewitt, Carson Keeter, Sara E Buckley, Kenneth J Hunt
{"title":"允诺:足部和踝关节手术的最小临床重要差异。","authors":"Nathaniel E Zona, Michael A Hewitt, Carson Keeter, Sara E Buckley, Kenneth J Hunt","doi":"10.1177/24730114251334055","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Minimal clinically important differences (MCIDs) increase patient-reported outcome measure (PROM) utility by defining benchmarks of meaningful improvement. The threshold for appreciable improvement may be unique to specific patient characteristics. To help establish benchmarks and improve evaluation of patient progress, this study investigates whether surgery type and demographic characteristics impact MCID.</p><p><strong>Methods: </strong>All foot and ankle patients within a single institution's PRO registry were screened. Patients without preoperative or ≥ 180-day follow-up in PROMIS physical function (PF) Computer Adaptive Test (CAT) (v2.0) and pain interference (PI) CAT (v1.1) were excluded. Foot and Ankle Single Assessment Numeric Evaluation (FA SANE) was used as an anchor for MCID calculations. MCID was compared across 11 foot and ankle surgical categories, reported sex, body mass index (BMI), and social deprivation index (SDI).</p><p><strong>Results: </strong>We included 1243 patients with an average follow-up of 456 ± 176 days. Patients significantly improved in PF by 8.2 ± 10.9 (<i>P</i> < .001) and PI by -8.1 ± 9.5 (<i>P</i> < .001). Global MCID estimates for PF and PI were 5.5 (95% CI 4.9, 6.0) and -5.8 (95% CI -5.3, -6.3), respectively, when anchored against FA SANE. The MCIDs using a ½ SD distribution-based method were 5.5 and -4.8, respectively. Surgery type greatly affected MCID, ranging from 2.3 and -3.8 for hardware removals to 15.7 and -9.8 for small soft tissue surgeries. MCID differences across reported sex, BMI, and SDI never exceeded 1.9 points.</p><p><strong>Conclusion: </strong>A 6-month postoperative improvement of ≥ 5.5 and ≤ -4.8 in PROMIS PF and PI suggest meaningful clinical differences from baseline. However, MCID values for PROMIS scales vary across foot and ankle surgeries and patient characteristics, suggesting a global MCID for patient populations may not reflect the true threshold of meaningful change for each individual patient. Anchoring to FA SANE allows physicians to more objectively gauge appreciable change in patient-specific contexts.</p><p><strong>Level of evidence: </strong>Level III, retrospective cohort study.</p>","PeriodicalId":12429,"journal":{"name":"Foot & Ankle Orthopaedics","volume":"10 2","pages":"24730114251334055"},"PeriodicalIF":0.0000,"publicationDate":"2025-05-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12049601/pdf/","citationCount":"0","resultStr":"{\"title\":\"PROMIS Minimal Clinically Important Differences Across Foot and Ankle Surgeries.\",\"authors\":\"Nathaniel E Zona, Michael A Hewitt, Carson Keeter, Sara E Buckley, Kenneth J Hunt\",\"doi\":\"10.1177/24730114251334055\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Minimal clinically important differences (MCIDs) increase patient-reported outcome measure (PROM) utility by defining benchmarks of meaningful improvement. The threshold for appreciable improvement may be unique to specific patient characteristics. To help establish benchmarks and improve evaluation of patient progress, this study investigates whether surgery type and demographic characteristics impact MCID.</p><p><strong>Methods: </strong>All foot and ankle patients within a single institution's PRO registry were screened. Patients without preoperative or ≥ 180-day follow-up in PROMIS physical function (PF) Computer Adaptive Test (CAT) (v2.0) and pain interference (PI) CAT (v1.1) were excluded. Foot and Ankle Single Assessment Numeric Evaluation (FA SANE) was used as an anchor for MCID calculations. MCID was compared across 11 foot and ankle surgical categories, reported sex, body mass index (BMI), and social deprivation index (SDI).</p><p><strong>Results: </strong>We included 1243 patients with an average follow-up of 456 ± 176 days. Patients significantly improved in PF by 8.2 ± 10.9 (<i>P</i> < .001) and PI by -8.1 ± 9.5 (<i>P</i> < .001). Global MCID estimates for PF and PI were 5.5 (95% CI 4.9, 6.0) and -5.8 (95% CI -5.3, -6.3), respectively, when anchored against FA SANE. The MCIDs using a ½ SD distribution-based method were 5.5 and -4.8, respectively. Surgery type greatly affected MCID, ranging from 2.3 and -3.8 for hardware removals to 15.7 and -9.8 for small soft tissue surgeries. MCID differences across reported sex, BMI, and SDI never exceeded 1.9 points.</p><p><strong>Conclusion: </strong>A 6-month postoperative improvement of ≥ 5.5 and ≤ -4.8 in PROMIS PF and PI suggest meaningful clinical differences from baseline. However, MCID values for PROMIS scales vary across foot and ankle surgeries and patient characteristics, suggesting a global MCID for patient populations may not reflect the true threshold of meaningful change for each individual patient. Anchoring to FA SANE allows physicians to more objectively gauge appreciable change in patient-specific contexts.</p><p><strong>Level of evidence: </strong>Level III, retrospective cohort study.</p>\",\"PeriodicalId\":12429,\"journal\":{\"name\":\"Foot & Ankle Orthopaedics\",\"volume\":\"10 2\",\"pages\":\"24730114251334055\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2025-05-02\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12049601/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Foot & Ankle Orthopaedics\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1177/24730114251334055\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/4/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Foot & Ankle Orthopaedics","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/24730114251334055","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/4/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
PROMIS Minimal Clinically Important Differences Across Foot and Ankle Surgeries.
Background: Minimal clinically important differences (MCIDs) increase patient-reported outcome measure (PROM) utility by defining benchmarks of meaningful improvement. The threshold for appreciable improvement may be unique to specific patient characteristics. To help establish benchmarks and improve evaluation of patient progress, this study investigates whether surgery type and demographic characteristics impact MCID.
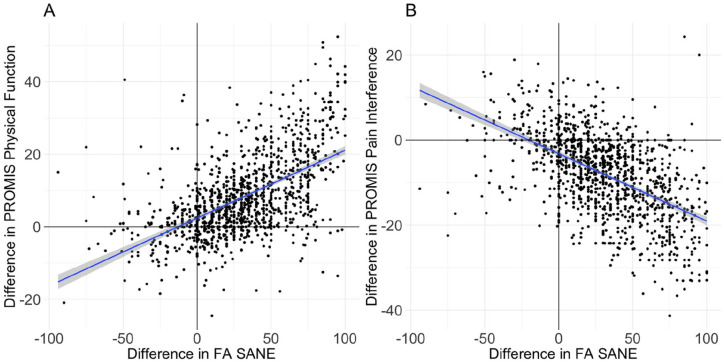
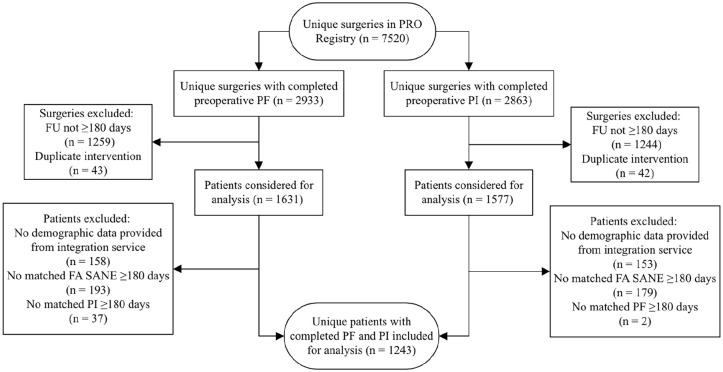
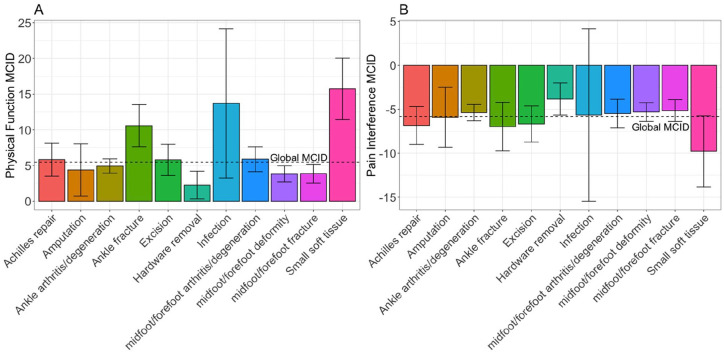
Methods: All foot and ankle patients within a single institution's PRO registry were screened. Patients without preoperative or ≥ 180-day follow-up in PROMIS physical function (PF) Computer Adaptive Test (CAT) (v2.0) and pain interference (PI) CAT (v1.1) were excluded. Foot and Ankle Single Assessment Numeric Evaluation (FA SANE) was used as an anchor for MCID calculations. MCID was compared across 11 foot and ankle surgical categories, reported sex, body mass index (BMI), and social deprivation index (SDI).
Results: We included 1243 patients with an average follow-up of 456 ± 176 days. Patients significantly improved in PF by 8.2 ± 10.9 (P < .001) and PI by -8.1 ± 9.5 (P < .001). Global MCID estimates for PF and PI were 5.5 (95% CI 4.9, 6.0) and -5.8 (95% CI -5.3, -6.3), respectively, when anchored against FA SANE. The MCIDs using a ½ SD distribution-based method were 5.5 and -4.8, respectively. Surgery type greatly affected MCID, ranging from 2.3 and -3.8 for hardware removals to 15.7 and -9.8 for small soft tissue surgeries. MCID differences across reported sex, BMI, and SDI never exceeded 1.9 points.
Conclusion: A 6-month postoperative improvement of ≥ 5.5 and ≤ -4.8 in PROMIS PF and PI suggest meaningful clinical differences from baseline. However, MCID values for PROMIS scales vary across foot and ankle surgeries and patient characteristics, suggesting a global MCID for patient populations may not reflect the true threshold of meaningful change for each individual patient. Anchoring to FA SANE allows physicians to more objectively gauge appreciable change in patient-specific contexts.
Level of evidence: Level III, retrospective cohort study.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


