Rachel M Nygaard, Emily Colonna, Rediat A Tilahun, Charly Vang, Gopal Punjabi, Alexandra Lacey, Kyle Schmitz, Derek C Lumbard
{"title":"到溶栓和组织挽救的时间:评估严重冻伤后的反应。","authors":"Rachel M Nygaard, Emily Colonna, Rediat A Tilahun, Charly Vang, Gopal Punjabi, Alexandra Lacey, Kyle Schmitz, Derek C Lumbard","doi":"10.1093/jbcr/iraf051","DOIUrl":null,"url":null,"abstract":"<p><p>Approximately 30% of severe frostbite injuries result in amputation. Thrombolytic therapy is used to reduce tissue loss following severe frostbite injury. This study evaluates factors impacting the effectiveness of thrombolytics using post-treatment perfusion imaging and amputation level as outcome measures. We hypothesize that categorizing thrombolytic-treated patients into full, partial, and nonresponders enable a nuanced evaluation of treatment effectiveness. A prospectively maintained frostbite database was reviewed for patients with post-rewarming perfusion deficits measured by Tc99 scans who received IV thrombolytics. Of 131 patients, 71% were full responders, 23.7% were partial responders, and 5.3% were nonresponders for surgical outcome. The median time to thrombolytics was 5.5 h (range 1-14.5) for full responders; 7 h (range 3.5-14) for partial responders; and 10 h (range 1.5-11.5) for nonresponders. Full responders exhibited smaller initial perfusion deficits. Psychosocial or comorbid factors were not significantly different across groups. Nonresponse was associated with a longer time to thrombolytics, larger perfusion deficits, and cellulitis/infection. Using imaging outcomes to reduce confounding by infection, 93 patients were evaluated: 28% were full responders, 57% were partial responders, and 15% were nonresponders. Full responders for imaging outcomes corresponded with surgical outcomes and had no amputations, while 37.7% of partial responders and 42.9% of nonresponders on imaging outcomes had amputations. This study is the largest to evaluate thrombolytic outcomes in severe frostbite-injured patients, showing nearly 95% of patients improve after thrombolytic treatment for severe frostbite injury. This provides new insight into thrombolytic responses and a novel assessment of thrombolytic treatment efficacy. These findings underscore the importance of timely thrombolytic administration and demonstrate benefits for patients treated outside the standard thrombolytic treatment windows.</p>","PeriodicalId":15205,"journal":{"name":"Journal of Burn Care & Research","volume":" ","pages":"730-740"},"PeriodicalIF":1.8000,"publicationDate":"2025-08-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12397684/pdf/","citationCount":"0","resultStr":"{\"title\":\"Time to Thrombolytics and Tissue Salvage: Assessing Response Following Severe Frostbite Injury.\",\"authors\":\"Rachel M Nygaard, Emily Colonna, Rediat A Tilahun, Charly Vang, Gopal Punjabi, Alexandra Lacey, Kyle Schmitz, Derek C Lumbard\",\"doi\":\"10.1093/jbcr/iraf051\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Approximately 30% of severe frostbite injuries result in amputation. Thrombolytic therapy is used to reduce tissue loss following severe frostbite injury. This study evaluates factors impacting the effectiveness of thrombolytics using post-treatment perfusion imaging and amputation level as outcome measures. We hypothesize that categorizing thrombolytic-treated patients into full, partial, and nonresponders enable a nuanced evaluation of treatment effectiveness. A prospectively maintained frostbite database was reviewed for patients with post-rewarming perfusion deficits measured by Tc99 scans who received IV thrombolytics. Of 131 patients, 71% were full responders, 23.7% were partial responders, and 5.3% were nonresponders for surgical outcome. The median time to thrombolytics was 5.5 h (range 1-14.5) for full responders; 7 h (range 3.5-14) for partial responders; and 10 h (range 1.5-11.5) for nonresponders. Full responders exhibited smaller initial perfusion deficits. Psychosocial or comorbid factors were not significantly different across groups. Nonresponse was associated with a longer time to thrombolytics, larger perfusion deficits, and cellulitis/infection. Using imaging outcomes to reduce confounding by infection, 93 patients were evaluated: 28% were full responders, 57% were partial responders, and 15% were nonresponders. Full responders for imaging outcomes corresponded with surgical outcomes and had no amputations, while 37.7% of partial responders and 42.9% of nonresponders on imaging outcomes had amputations. This study is the largest to evaluate thrombolytic outcomes in severe frostbite-injured patients, showing nearly 95% of patients improve after thrombolytic treatment for severe frostbite injury. This provides new insight into thrombolytic responses and a novel assessment of thrombolytic treatment efficacy. These findings underscore the importance of timely thrombolytic administration and demonstrate benefits for patients treated outside the standard thrombolytic treatment windows.</p>\",\"PeriodicalId\":15205,\"journal\":{\"name\":\"Journal of Burn Care & Research\",\"volume\":\" \",\"pages\":\"730-740\"},\"PeriodicalIF\":1.8000,\"publicationDate\":\"2025-08-30\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12397684/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Burn Care & Research\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1093/jbcr/iraf051\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"CRITICAL CARE MEDICINE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Burn Care & Research","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1093/jbcr/iraf051","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"CRITICAL CARE MEDICINE","Score":null,"Total":0}
Time to Thrombolytics and Tissue Salvage: Assessing Response Following Severe Frostbite Injury.
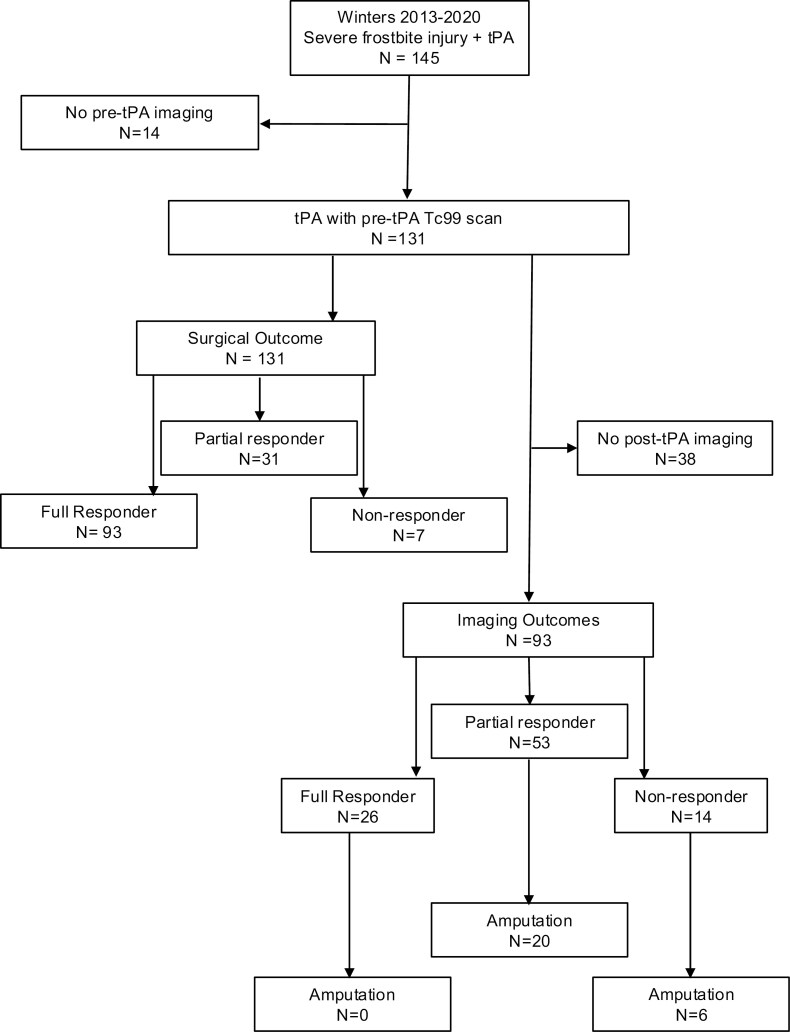
Approximately 30% of severe frostbite injuries result in amputation. Thrombolytic therapy is used to reduce tissue loss following severe frostbite injury. This study evaluates factors impacting the effectiveness of thrombolytics using post-treatment perfusion imaging and amputation level as outcome measures. We hypothesize that categorizing thrombolytic-treated patients into full, partial, and nonresponders enable a nuanced evaluation of treatment effectiveness. A prospectively maintained frostbite database was reviewed for patients with post-rewarming perfusion deficits measured by Tc99 scans who received IV thrombolytics. Of 131 patients, 71% were full responders, 23.7% were partial responders, and 5.3% were nonresponders for surgical outcome. The median time to thrombolytics was 5.5 h (range 1-14.5) for full responders; 7 h (range 3.5-14) for partial responders; and 10 h (range 1.5-11.5) for nonresponders. Full responders exhibited smaller initial perfusion deficits. Psychosocial or comorbid factors were not significantly different across groups. Nonresponse was associated with a longer time to thrombolytics, larger perfusion deficits, and cellulitis/infection. Using imaging outcomes to reduce confounding by infection, 93 patients were evaluated: 28% were full responders, 57% were partial responders, and 15% were nonresponders. Full responders for imaging outcomes corresponded with surgical outcomes and had no amputations, while 37.7% of partial responders and 42.9% of nonresponders on imaging outcomes had amputations. This study is the largest to evaluate thrombolytic outcomes in severe frostbite-injured patients, showing nearly 95% of patients improve after thrombolytic treatment for severe frostbite injury. This provides new insight into thrombolytic responses and a novel assessment of thrombolytic treatment efficacy. These findings underscore the importance of timely thrombolytic administration and demonstrate benefits for patients treated outside the standard thrombolytic treatment windows.
期刊介绍:
Journal of Burn Care & Research provides the latest information on advances in burn prevention, research, education, delivery of acute care, and research to all members of the burn care team. As the official publication of the American Burn Association, this is the only U.S. journal devoted exclusively to the treatment and research of patients with burns. Original, peer-reviewed articles present the latest information on surgical procedures, acute care, reconstruction, burn prevention, and research and education. Other topics include physical therapy/occupational therapy, nutrition, current events in the evolving healthcare debate, and reports on the newest computer software for diagnostics and treatment. The Journal serves all burn care specialists, from physicians, nurses, and physical and occupational therapists to psychologists, counselors, and researchers.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


