Grace R Fassina, Emily E Nguyen, David Cho, Drake J Williams, Alexander R Evans, Panayiotis E Pelargos, Christopher S Graffeo
{"title":"问号问题:半骨切除术后伤口愈合。","authors":"Grace R Fassina, Emily E Nguyen, David Cho, Drake J Williams, Alexander R Evans, Panayiotis E Pelargos, Christopher S Graffeo","doi":"10.1055/a-2561-7951","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>The reverse question mark (RQM) incision is the conventional scalp flap technique incorporated during decompressive hemicraniectomy (DHC) operations. Recently, the retroauricular (RA) incision emerged as a possible alternative. We sought to assess the contemporary literature regarding postoperative outcomes following RQM or RA for DHC and subsequent cranioplasty.</p><p><strong>Methods: </strong>MEDLINE and Embase databases were queried using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. Studies reporting outcomes after primary DHC and secondary cranioplasty for both RQM and RA were included in a meta-analysis of proportions performed using random-effects modeling.</p><p><strong>Results: </strong>Five manuscripts representing a total of 511 patients met the inclusion criteria. No difference was observed in the rate of primary surgical site infection (SSI) after RQM as compared with RA (OR = 1.64, 95% CI = 0.92-2.92). Similarly, based on those four studies reporting SSI data after cranioplasty, no difference was detected in secondary SSI rates between RQM and RA (OR = 1.93, 95% CI = 0.79-4.72). Patients who underwent primary RQM had increased odds of undergoing cranioplasty compared with patients who had received a primary RA (OR = 1.57, 95% CI = 1.03-2.39).</p><p><strong>Conclusion: </strong>This novel systematic review and meta-analysis reported postoperative outcomes after DHC using either the RQM or RA incision technique. No significant difference was noted in SSI after either the primary decompression or the secondary cranioplasty. These findings support the use of either technique in routine practice, as guided by surgeon preference or other clinical considerations, such as superficial temporal artery preservation for an unrelated future indication.</p>","PeriodicalId":44256,"journal":{"name":"Journal of Neurological Surgery Reports","volume":"86 2","pages":"e77-e82"},"PeriodicalIF":0.7000,"publicationDate":"2025-04-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12020538/pdf/","citationCount":"0","resultStr":"{\"title\":\"The Question Mark Question: Wound Healing after Hemicraniectomy.\",\"authors\":\"Grace R Fassina, Emily E Nguyen, David Cho, Drake J Williams, Alexander R Evans, Panayiotis E Pelargos, Christopher S Graffeo\",\"doi\":\"10.1055/a-2561-7951\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>The reverse question mark (RQM) incision is the conventional scalp flap technique incorporated during decompressive hemicraniectomy (DHC) operations. Recently, the retroauricular (RA) incision emerged as a possible alternative. We sought to assess the contemporary literature regarding postoperative outcomes following RQM or RA for DHC and subsequent cranioplasty.</p><p><strong>Methods: </strong>MEDLINE and Embase databases were queried using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. Studies reporting outcomes after primary DHC and secondary cranioplasty for both RQM and RA were included in a meta-analysis of proportions performed using random-effects modeling.</p><p><strong>Results: </strong>Five manuscripts representing a total of 511 patients met the inclusion criteria. No difference was observed in the rate of primary surgical site infection (SSI) after RQM as compared with RA (OR = 1.64, 95% CI = 0.92-2.92). Similarly, based on those four studies reporting SSI data after cranioplasty, no difference was detected in secondary SSI rates between RQM and RA (OR = 1.93, 95% CI = 0.79-4.72). Patients who underwent primary RQM had increased odds of undergoing cranioplasty compared with patients who had received a primary RA (OR = 1.57, 95% CI = 1.03-2.39).</p><p><strong>Conclusion: </strong>This novel systematic review and meta-analysis reported postoperative outcomes after DHC using either the RQM or RA incision technique. No significant difference was noted in SSI after either the primary decompression or the secondary cranioplasty. These findings support the use of either technique in routine practice, as guided by surgeon preference or other clinical considerations, such as superficial temporal artery preservation for an unrelated future indication.</p>\",\"PeriodicalId\":44256,\"journal\":{\"name\":\"Journal of Neurological Surgery Reports\",\"volume\":\"86 2\",\"pages\":\"e77-e82\"},\"PeriodicalIF\":0.7000,\"publicationDate\":\"2025-04-09\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12020538/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Neurological Surgery Reports\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1055/a-2561-7951\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/4/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q4\",\"JCRName\":\"CLINICAL NEUROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Neurological Surgery Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1055/a-2561-7951","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/4/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
摘要
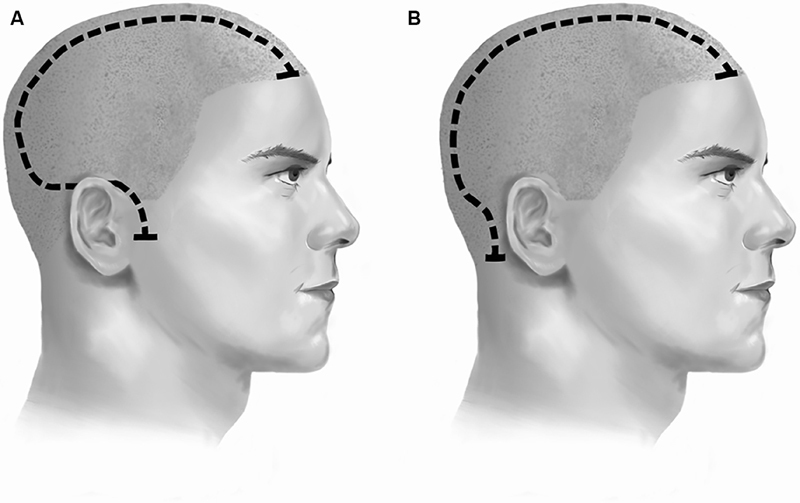
反向问号(RQM)切口是在减压性半颅骨切除术(DHC)手术中采用的常规头皮皮瓣技术。最近,耳后(RA)切口成为一种可能的选择。我们试图评估有关RQM或RA治疗DHC和随后颅骨成形术的术后结果的当代文献。方法:使用系统评价和荟萃分析首选报告项目(PRISMA)指南对MEDLINE和Embase数据库进行查询。报告RQM和RA的原发性DHC和二次颅骨成形术后的结果的研究被纳入使用随机效应模型进行的比例荟萃分析。结果:5篇文献共511例患者符合纳入标准。与RA相比,RQM术后原发性手术部位感染(SSI)发生率无差异(OR = 1.64, 95% CI = 0.92-2.92)。同样,基于报告颅骨成形术后SSI数据的四项研究,RQM和RA在继发性SSI发生率方面没有发现差异(OR = 1.93, 95% CI = 0.79-4.72)。与接受原发性RA的患者相比,接受原发性RQM的患者接受颅骨成形术的几率增加(OR = 1.57, 95% CI = 1.03-2.39)。结论:这项新颖的系统评价和荟萃分析报告了采用RQM或RA切口技术的DHC术后结果。无论是初次减压还是二次颅骨成形术,SSI均无显著差异。这些发现支持在常规实践中使用这两种技术,根据外科医生的偏好或其他临床考虑,如为不相关的未来适应症保留颞浅动脉。
The Question Mark Question: Wound Healing after Hemicraniectomy.
Introduction: The reverse question mark (RQM) incision is the conventional scalp flap technique incorporated during decompressive hemicraniectomy (DHC) operations. Recently, the retroauricular (RA) incision emerged as a possible alternative. We sought to assess the contemporary literature regarding postoperative outcomes following RQM or RA for DHC and subsequent cranioplasty.
Methods: MEDLINE and Embase databases were queried using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. Studies reporting outcomes after primary DHC and secondary cranioplasty for both RQM and RA were included in a meta-analysis of proportions performed using random-effects modeling.
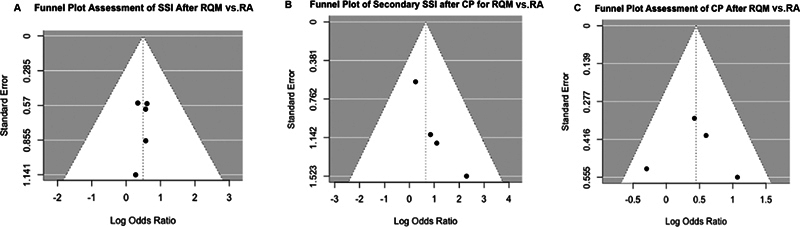
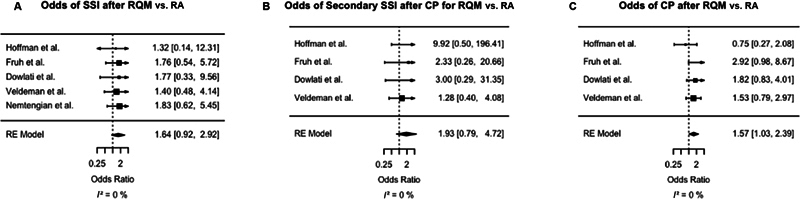
Results: Five manuscripts representing a total of 511 patients met the inclusion criteria. No difference was observed in the rate of primary surgical site infection (SSI) after RQM as compared with RA (OR = 1.64, 95% CI = 0.92-2.92). Similarly, based on those four studies reporting SSI data after cranioplasty, no difference was detected in secondary SSI rates between RQM and RA (OR = 1.93, 95% CI = 0.79-4.72). Patients who underwent primary RQM had increased odds of undergoing cranioplasty compared with patients who had received a primary RA (OR = 1.57, 95% CI = 1.03-2.39).
Conclusion: This novel systematic review and meta-analysis reported postoperative outcomes after DHC using either the RQM or RA incision technique. No significant difference was noted in SSI after either the primary decompression or the secondary cranioplasty. These findings support the use of either technique in routine practice, as guided by surgeon preference or other clinical considerations, such as superficial temporal artery preservation for an unrelated future indication.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


