Syed Faqeer Hussain Bokhari, Muhammad Muaz Mushtaq, Maham Mushtaq, Husnain Ali, Danyal Bakht, Muhayya Faizullah, Almas Asghar, Muhammad Khan Buhadur Ali, Muhammad Asad Sarwar, Maryyam Liaqat, Asma Iqbal, Wahidullah Dost
{"title":"伊伐布雷定治疗先天性结缔性异位心动过速:系统综述。","authors":"Syed Faqeer Hussain Bokhari, Muhammad Muaz Mushtaq, Maham Mushtaq, Husnain Ali, Danyal Bakht, Muhayya Faizullah, Almas Asghar, Muhammad Khan Buhadur Ali, Muhammad Asad Sarwar, Maryyam Liaqat, Asma Iqbal, Wahidullah Dost","doi":"10.4330/wjc.v17.i4.104465","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Congenital junctional ectopic tachycardia (CJET) is a rare but life-threatening arrhythmia in neonates and infants, often refractory to conventional antiarrhythmic therapy. Ivabradine, a selective inhibitor of hyperpolarization-activated cyclic nucleotide-gated channels, has emerged as a promising drug for CJET management.</p><p><strong>Aim: </strong>To evaluate the efficacy and safety of ivabradine in the management of CJET. Specifically, this study aims to analyze the dosing strategies, treatment outcomes, and the role of ivabradine as monotherapy or adjunct therapy in patients who have previously received other antiarrhythmic medications. Additionally, this review seeks to assess the impact of ivabradine on heart rate (HR) control, rhythm conversion, and its overall safety profile to provide evidence-based insights into its clinical use for CJET management.</p><p><strong>Methods: </strong>This systematic review aims to evaluate the outcomes of ivabradine, either as monotherapy or as an adjunctive therapy, in the treatment of CJET. A comprehensive literature search was conducted across multiple electronic databases to identify relevant studies investigating the use of ivabradine in CJET. Stringent inclusion and exclusion criteria were applied to ensure the inclusion of high-quality, peer-reviewed studies. Data extraction and quality assessment were performed independently by two reviewers.</p><p><strong>Results: </strong>Ten studies, comprising 6 case reports, 3 case series, and 1 cohort study, met the inclusion criteria. Ivabradine doses ranged from 0.025 to 0.28 mg/kg/dose, administered either as monotherapy or in combination with various antiarrhythmic medications. Overall, ivabradine demonstrated promising results in achieving HR control, conversion to sinus rhythm, or stabilization of junctional rhythm. No significant adverse effects related to ivabradine were reported.</p><p><strong>Conclusion: </strong>The available evidence suggests that ivabradine may be an effective adjunctive therapy or, in some cases, a potential monotherapy for the management of CJET, particularly in cases refractory to traditional antiarrhythmic medications. However, the current evidence is limited by the small sample sizes and retrospective nature of the included studies. Well-designed prospective studies with larger cohorts and longer follow-up periods are warranted to further elucidate the role of ivabradine in CJET management.</p>","PeriodicalId":23800,"journal":{"name":"World Journal of Cardiology","volume":"17 4","pages":"104465"},"PeriodicalIF":2.8000,"publicationDate":"2025-04-26","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12038696/pdf/","citationCount":"0","resultStr":"{\"title\":\"Ivabradine in the treatment of congenital junctional ectopic tachycardia: A systematic review.\",\"authors\":\"Syed Faqeer Hussain Bokhari, Muhammad Muaz Mushtaq, Maham Mushtaq, Husnain Ali, Danyal Bakht, Muhayya Faizullah, Almas Asghar, Muhammad Khan Buhadur Ali, Muhammad Asad Sarwar, Maryyam Liaqat, Asma Iqbal, Wahidullah Dost\",\"doi\":\"10.4330/wjc.v17.i4.104465\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Congenital junctional ectopic tachycardia (CJET) is a rare but life-threatening arrhythmia in neonates and infants, often refractory to conventional antiarrhythmic therapy. Ivabradine, a selective inhibitor of hyperpolarization-activated cyclic nucleotide-gated channels, has emerged as a promising drug for CJET management.</p><p><strong>Aim: </strong>To evaluate the efficacy and safety of ivabradine in the management of CJET. Specifically, this study aims to analyze the dosing strategies, treatment outcomes, and the role of ivabradine as monotherapy or adjunct therapy in patients who have previously received other antiarrhythmic medications. Additionally, this review seeks to assess the impact of ivabradine on heart rate (HR) control, rhythm conversion, and its overall safety profile to provide evidence-based insights into its clinical use for CJET management.</p><p><strong>Methods: </strong>This systematic review aims to evaluate the outcomes of ivabradine, either as monotherapy or as an adjunctive therapy, in the treatment of CJET. A comprehensive literature search was conducted across multiple electronic databases to identify relevant studies investigating the use of ivabradine in CJET. Stringent inclusion and exclusion criteria were applied to ensure the inclusion of high-quality, peer-reviewed studies. Data extraction and quality assessment were performed independently by two reviewers.</p><p><strong>Results: </strong>Ten studies, comprising 6 case reports, 3 case series, and 1 cohort study, met the inclusion criteria. Ivabradine doses ranged from 0.025 to 0.28 mg/kg/dose, administered either as monotherapy or in combination with various antiarrhythmic medications. Overall, ivabradine demonstrated promising results in achieving HR control, conversion to sinus rhythm, or stabilization of junctional rhythm. No significant adverse effects related to ivabradine were reported.</p><p><strong>Conclusion: </strong>The available evidence suggests that ivabradine may be an effective adjunctive therapy or, in some cases, a potential monotherapy for the management of CJET, particularly in cases refractory to traditional antiarrhythmic medications. However, the current evidence is limited by the small sample sizes and retrospective nature of the included studies. Well-designed prospective studies with larger cohorts and longer follow-up periods are warranted to further elucidate the role of ivabradine in CJET management.</p>\",\"PeriodicalId\":23800,\"journal\":{\"name\":\"World Journal of Cardiology\",\"volume\":\"17 4\",\"pages\":\"104465\"},\"PeriodicalIF\":2.8000,\"publicationDate\":\"2025-04-26\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12038696/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"World Journal of Cardiology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.4330/wjc.v17.i4.104465\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"World Journal of Cardiology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4330/wjc.v17.i4.104465","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
Ivabradine in the treatment of congenital junctional ectopic tachycardia: A systematic review.
Background: Congenital junctional ectopic tachycardia (CJET) is a rare but life-threatening arrhythmia in neonates and infants, often refractory to conventional antiarrhythmic therapy. Ivabradine, a selective inhibitor of hyperpolarization-activated cyclic nucleotide-gated channels, has emerged as a promising drug for CJET management.
Aim: To evaluate the efficacy and safety of ivabradine in the management of CJET. Specifically, this study aims to analyze the dosing strategies, treatment outcomes, and the role of ivabradine as monotherapy or adjunct therapy in patients who have previously received other antiarrhythmic medications. Additionally, this review seeks to assess the impact of ivabradine on heart rate (HR) control, rhythm conversion, and its overall safety profile to provide evidence-based insights into its clinical use for CJET management.
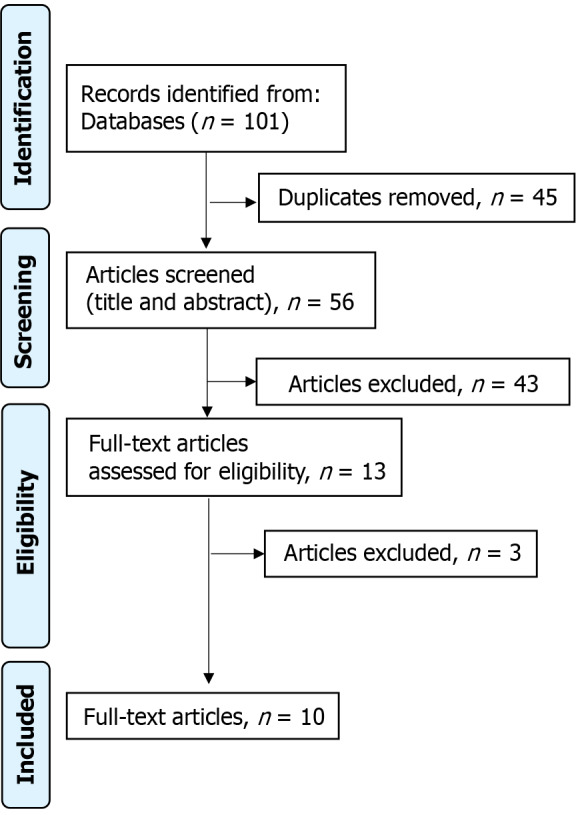
Methods: This systematic review aims to evaluate the outcomes of ivabradine, either as monotherapy or as an adjunctive therapy, in the treatment of CJET. A comprehensive literature search was conducted across multiple electronic databases to identify relevant studies investigating the use of ivabradine in CJET. Stringent inclusion and exclusion criteria were applied to ensure the inclusion of high-quality, peer-reviewed studies. Data extraction and quality assessment were performed independently by two reviewers.
Results: Ten studies, comprising 6 case reports, 3 case series, and 1 cohort study, met the inclusion criteria. Ivabradine doses ranged from 0.025 to 0.28 mg/kg/dose, administered either as monotherapy or in combination with various antiarrhythmic medications. Overall, ivabradine demonstrated promising results in achieving HR control, conversion to sinus rhythm, or stabilization of junctional rhythm. No significant adverse effects related to ivabradine were reported.
Conclusion: The available evidence suggests that ivabradine may be an effective adjunctive therapy or, in some cases, a potential monotherapy for the management of CJET, particularly in cases refractory to traditional antiarrhythmic medications. However, the current evidence is limited by the small sample sizes and retrospective nature of the included studies. Well-designed prospective studies with larger cohorts and longer follow-up periods are warranted to further elucidate the role of ivabradine in CJET management.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


