{"title":"急性伴慢性肝衰竭患者死亡率的预后因素。","authors":"Huijie Jiang, Zhihao Zhao, Shiyu Cui, Xianggen Kong, Xuemei Jiang","doi":"10.1097/MEG.0000000000002958","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>The aim is to explore significant prognostic factors for 90-day mortality in patients with acute-on-chronic liver failure (ACLF) and assist clinicians in the early identification of critically ill ACLF patients.</p><p><strong>Methods: </strong>A retrospective analysis was conducted on 288 ACLF patients, who were classified into survivors ( n = 187) and nonsurvivors ( n = 101) based on 90-day outcomes. Multivariate stepwise logistic regression analyses were employed to identify significant prognostic factors and construct a novel prognostic model, the AHUCTPI. The model's performance was assessed and the internal validation was performed. Additionally, the influence of dynamic changes in laboratory markers on 90-day mortality was examined.</p><p><strong>Results: </strong>Independent risk factors for 90-day mortality included age ≥45 years, presence of hepatic encephalopathy (HE), and upper gastrointestinal bleeding (UGB) during hospitalization, imaging-confirmed cirrhosis at admission, elevated baseline total bilirubin (TBIL), reduced baseline platelet-to-neutrophil ratio (PNR), and elevated baseline international normalized ratio (INR) ( P < 0.05 for all). The AHUCTPI model's formula is as follows: Logit ( p ) = -10.019 + 1.808 × age (1 if ≥45 years, 0 if <45 years) + 1.048 × HE (1 if present, 0 if absent) + 1.721 × UGB (1 if present, 0 if absent) + 1.362 × cirrhosis (1 if present, 0 if absent) + 0.008 × TBIL (μmol/L) - 0.039 × PNR + 1.963 × INR. The AUHCTPI model demonstrated superior predictive accuracy compared with the MELD (Model for End-Stage Liver Disease) score, with the area under the receiver operating characteristic curve values of 0.914 and 0.739, respectively, and calibration curves closely approximating the ideal curve.</p><p><strong>Conclusion: </strong>ACLF is a complex, dynamic syndrome. Age, HE, and UGB during hospitalization, imaging-diagnosed cirrhosis at admission, baseline TBIL, PNR, and INR were significant predictors for 90-day mortality in ACLF patients, and the AHUCTPI model provides excellent calibration and discrimination. Dynamic monitoring of laboratory trends enhances prognostic accuracy and supports timely clinical decision-making.</p>","PeriodicalId":11999,"journal":{"name":"European Journal of Gastroenterology & Hepatology","volume":" ","pages":"833-843"},"PeriodicalIF":1.8000,"publicationDate":"2025-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12122091/pdf/","citationCount":"0","resultStr":"{\"title\":\"Prognostic factors for mortality in patients with acute-on-chronic liver failure.\",\"authors\":\"Huijie Jiang, Zhihao Zhao, Shiyu Cui, Xianggen Kong, Xuemei Jiang\",\"doi\":\"10.1097/MEG.0000000000002958\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>The aim is to explore significant prognostic factors for 90-day mortality in patients with acute-on-chronic liver failure (ACLF) and assist clinicians in the early identification of critically ill ACLF patients.</p><p><strong>Methods: </strong>A retrospective analysis was conducted on 288 ACLF patients, who were classified into survivors ( n = 187) and nonsurvivors ( n = 101) based on 90-day outcomes. Multivariate stepwise logistic regression analyses were employed to identify significant prognostic factors and construct a novel prognostic model, the AHUCTPI. The model's performance was assessed and the internal validation was performed. Additionally, the influence of dynamic changes in laboratory markers on 90-day mortality was examined.</p><p><strong>Results: </strong>Independent risk factors for 90-day mortality included age ≥45 years, presence of hepatic encephalopathy (HE), and upper gastrointestinal bleeding (UGB) during hospitalization, imaging-confirmed cirrhosis at admission, elevated baseline total bilirubin (TBIL), reduced baseline platelet-to-neutrophil ratio (PNR), and elevated baseline international normalized ratio (INR) ( P < 0.05 for all). The AHUCTPI model's formula is as follows: Logit ( p ) = -10.019 + 1.808 × age (1 if ≥45 years, 0 if <45 years) + 1.048 × HE (1 if present, 0 if absent) + 1.721 × UGB (1 if present, 0 if absent) + 1.362 × cirrhosis (1 if present, 0 if absent) + 0.008 × TBIL (μmol/L) - 0.039 × PNR + 1.963 × INR. The AUHCTPI model demonstrated superior predictive accuracy compared with the MELD (Model for End-Stage Liver Disease) score, with the area under the receiver operating characteristic curve values of 0.914 and 0.739, respectively, and calibration curves closely approximating the ideal curve.</p><p><strong>Conclusion: </strong>ACLF is a complex, dynamic syndrome. Age, HE, and UGB during hospitalization, imaging-diagnosed cirrhosis at admission, baseline TBIL, PNR, and INR were significant predictors for 90-day mortality in ACLF patients, and the AHUCTPI model provides excellent calibration and discrimination. Dynamic monitoring of laboratory trends enhances prognostic accuracy and supports timely clinical decision-making.</p>\",\"PeriodicalId\":11999,\"journal\":{\"name\":\"European Journal of Gastroenterology & Hepatology\",\"volume\":\" \",\"pages\":\"833-843\"},\"PeriodicalIF\":1.8000,\"publicationDate\":\"2025-07-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12122091/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"European Journal of Gastroenterology & Hepatology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1097/MEG.0000000000002958\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/5/28 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"European Journal of Gastroenterology & Hepatology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1097/MEG.0000000000002958","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/5/28 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
Prognostic factors for mortality in patients with acute-on-chronic liver failure.
Objective: The aim is to explore significant prognostic factors for 90-day mortality in patients with acute-on-chronic liver failure (ACLF) and assist clinicians in the early identification of critically ill ACLF patients.
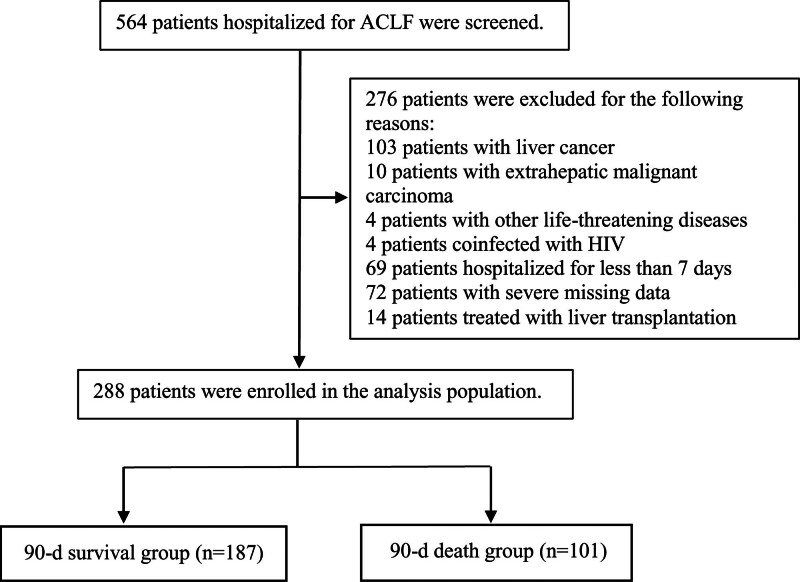
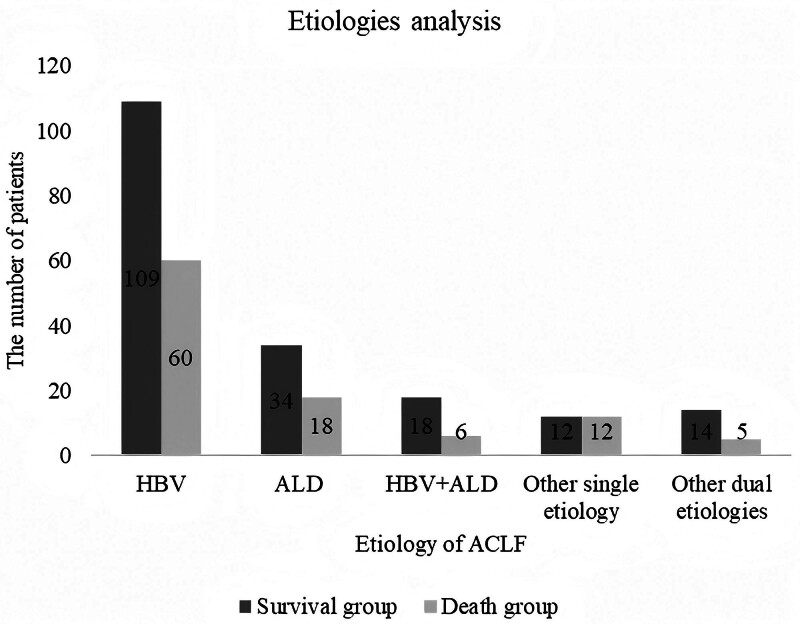
Methods: A retrospective analysis was conducted on 288 ACLF patients, who were classified into survivors ( n = 187) and nonsurvivors ( n = 101) based on 90-day outcomes. Multivariate stepwise logistic regression analyses were employed to identify significant prognostic factors and construct a novel prognostic model, the AHUCTPI. The model's performance was assessed and the internal validation was performed. Additionally, the influence of dynamic changes in laboratory markers on 90-day mortality was examined.
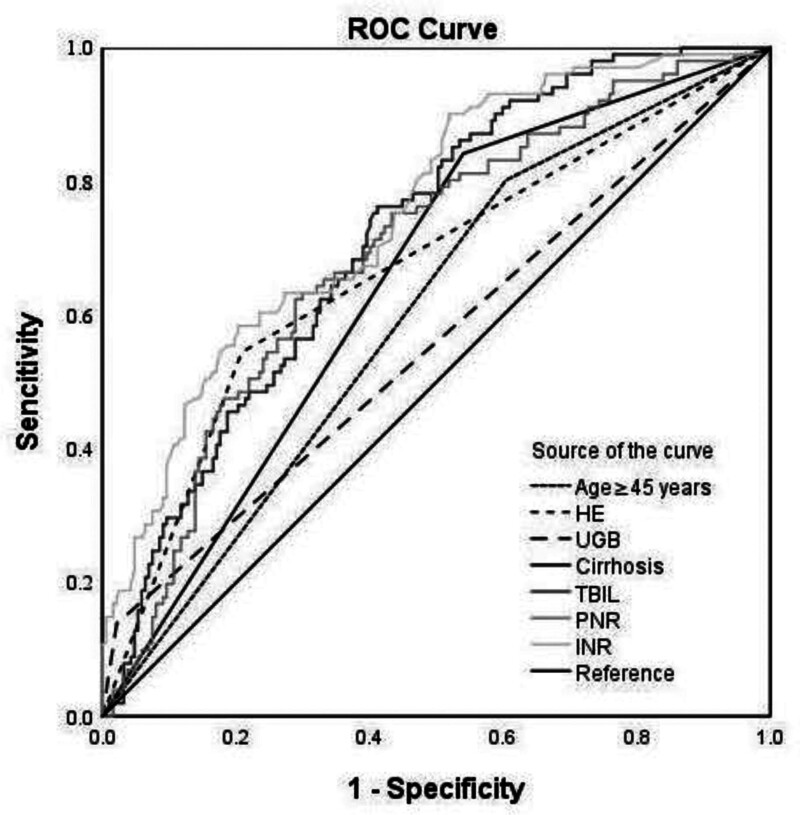
Results: Independent risk factors for 90-day mortality included age ≥45 years, presence of hepatic encephalopathy (HE), and upper gastrointestinal bleeding (UGB) during hospitalization, imaging-confirmed cirrhosis at admission, elevated baseline total bilirubin (TBIL), reduced baseline platelet-to-neutrophil ratio (PNR), and elevated baseline international normalized ratio (INR) ( P < 0.05 for all). The AHUCTPI model's formula is as follows: Logit ( p ) = -10.019 + 1.808 × age (1 if ≥45 years, 0 if <45 years) + 1.048 × HE (1 if present, 0 if absent) + 1.721 × UGB (1 if present, 0 if absent) + 1.362 × cirrhosis (1 if present, 0 if absent) + 0.008 × TBIL (μmol/L) - 0.039 × PNR + 1.963 × INR. The AUHCTPI model demonstrated superior predictive accuracy compared with the MELD (Model for End-Stage Liver Disease) score, with the area under the receiver operating characteristic curve values of 0.914 and 0.739, respectively, and calibration curves closely approximating the ideal curve.
Conclusion: ACLF is a complex, dynamic syndrome. Age, HE, and UGB during hospitalization, imaging-diagnosed cirrhosis at admission, baseline TBIL, PNR, and INR were significant predictors for 90-day mortality in ACLF patients, and the AHUCTPI model provides excellent calibration and discrimination. Dynamic monitoring of laboratory trends enhances prognostic accuracy and supports timely clinical decision-making.
期刊介绍:
European Journal of Gastroenterology & Hepatology publishes papers reporting original clinical and scientific research which are of a high standard and which contribute to the advancement of knowledge in the field of gastroenterology and hepatology.
The journal publishes three types of manuscript: in-depth reviews (by invitation only), full papers and case reports. Manuscripts submitted to the journal will be accepted on the understanding that the author has not previously submitted the paper to another journal or had the material published elsewhere. Authors are asked to disclose any affiliations, including financial, consultant, or institutional associations, that might lead to bias or a conflict of interest.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


