{"title":"支架辅助盘绕破裂颅内动脉瘤的安全性和有效性:单中心研究。","authors":"Deng-Xiang Zhang, Chao-Bao Luo, Chien-Hui Lee","doi":"10.4103/tcmj.tcmj_92_24","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>Endovascular coiling is a minimally invasive method to manage intracranial aneurysms. However, patients who undergo stent-assisted coiling (SAC) for acutely ruptured intracranial aneurysms need dual antiplatelet treatment. We reported our experience and outcomes of SAC for ruptured intracranial aneurysm.</p><p><strong>Materials and methods: </strong>We retrospectively collected data on procedure-related complications, rates of aneurysm rebleeding and recurrence, and clinical outcomes of patients with ruptured aneurysms managed by SAC over 2 years.</p><p><strong>Results: </strong>Among the 17 patients included in this study, there were 14 (82.4%) women and 3 (17.6%) men, with a mean age of 58.59 years (standard deviation = 13.57; range: 40-82 years). There were no periprocedural hemorrhagic complications and no aneurysm rebleeding before discharge. However, two patients developed acute brain infarction because of symptomatic vasospasm. Linear regression revealed significant associations of posterior circulation involvement with the Glasgow Outcome Score and modified Rankin Scale (mRS) at discharge and 6 months after. Besides, Hunt and Hess grade ≥3 has a significant association with mRS at discharge, 6 months, and 1 year after.</p><p><strong>Conclusion: </strong>SAC for ruptured aneurysm was technically feasible and did not carry an additional risk of postoperative aneurysm rebleeding secondary to antiplatelet treatment. Moreover, it had relatively low rates of aneurysm regrowth and coil compaction. Therefore, it can be a safe and effective endovascular treatment for acutely ruptured intracranial aneurysm.</p>","PeriodicalId":45873,"journal":{"name":"Tzu Chi Medical Journal","volume":"37 2","pages":"189-197"},"PeriodicalIF":1.6000,"publicationDate":"2024-08-12","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12048123/pdf/","citationCount":"0","resultStr":"{\"title\":\"Safety and efficacy of stent-assisted coiling ruptured intracranial aneurysms: A single-center experience.\",\"authors\":\"Deng-Xiang Zhang, Chao-Bao Luo, Chien-Hui Lee\",\"doi\":\"10.4103/tcmj.tcmj_92_24\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objectives: </strong>Endovascular coiling is a minimally invasive method to manage intracranial aneurysms. However, patients who undergo stent-assisted coiling (SAC) for acutely ruptured intracranial aneurysms need dual antiplatelet treatment. We reported our experience and outcomes of SAC for ruptured intracranial aneurysm.</p><p><strong>Materials and methods: </strong>We retrospectively collected data on procedure-related complications, rates of aneurysm rebleeding and recurrence, and clinical outcomes of patients with ruptured aneurysms managed by SAC over 2 years.</p><p><strong>Results: </strong>Among the 17 patients included in this study, there were 14 (82.4%) women and 3 (17.6%) men, with a mean age of 58.59 years (standard deviation = 13.57; range: 40-82 years). There were no periprocedural hemorrhagic complications and no aneurysm rebleeding before discharge. However, two patients developed acute brain infarction because of symptomatic vasospasm. Linear regression revealed significant associations of posterior circulation involvement with the Glasgow Outcome Score and modified Rankin Scale (mRS) at discharge and 6 months after. Besides, Hunt and Hess grade ≥3 has a significant association with mRS at discharge, 6 months, and 1 year after.</p><p><strong>Conclusion: </strong>SAC for ruptured aneurysm was technically feasible and did not carry an additional risk of postoperative aneurysm rebleeding secondary to antiplatelet treatment. Moreover, it had relatively low rates of aneurysm regrowth and coil compaction. Therefore, it can be a safe and effective endovascular treatment for acutely ruptured intracranial aneurysm.</p>\",\"PeriodicalId\":45873,\"journal\":{\"name\":\"Tzu Chi Medical Journal\",\"volume\":\"37 2\",\"pages\":\"189-197\"},\"PeriodicalIF\":1.6000,\"publicationDate\":\"2024-08-12\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12048123/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Tzu Chi Medical Journal\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.4103/tcmj.tcmj_92_24\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/4/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"MEDICINE, GENERAL & INTERNAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Tzu Chi Medical Journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4103/tcmj.tcmj_92_24","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/4/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
摘要
目的:血管内盘绕术是治疗颅内动脉瘤的一种微创方法。然而,接受支架辅助盘绕(SAC)治疗急性破裂颅内动脉瘤的患者需要双重抗血小板治疗。我们报告了SAC治疗颅内动脉瘤破裂的经验和结果。材料和方法:我们回顾性收集了手术相关并发症、动脉瘤再出血和复发率以及SAC治疗2年以上动脉瘤破裂患者的临床结果的数据。结果:本研究纳入的17例患者中,女性14例(82.4%),男性3例(17.6%),平均年龄58.59岁(标准差= 13.57;范围:40-82年)。出院前无围手术期出血并发症及动脉瘤再出血。然而,2例患者因症状性血管痉挛而发生急性脑梗死。线性回归显示,出院时和6个月后,后循环受累程度与格拉斯哥预后评分和改良兰金量表(mRS)有显著相关性。此外,Hunt and Hess分级≥3与出院时、6个月和1年后的mRS有显著相关。结论:SAC治疗破裂动脉瘤在技术上是可行的,并且不会带来抗血小板治疗后动脉瘤再出血的额外风险。此外,它的动脉瘤再生和线圈压实率相对较低。因此,它是一种安全有效的治疗急性颅内动脉瘤破裂的血管内治疗方法。
Safety and efficacy of stent-assisted coiling ruptured intracranial aneurysms: A single-center experience.
Objectives: Endovascular coiling is a minimally invasive method to manage intracranial aneurysms. However, patients who undergo stent-assisted coiling (SAC) for acutely ruptured intracranial aneurysms need dual antiplatelet treatment. We reported our experience and outcomes of SAC for ruptured intracranial aneurysm.
Materials and methods: We retrospectively collected data on procedure-related complications, rates of aneurysm rebleeding and recurrence, and clinical outcomes of patients with ruptured aneurysms managed by SAC over 2 years.
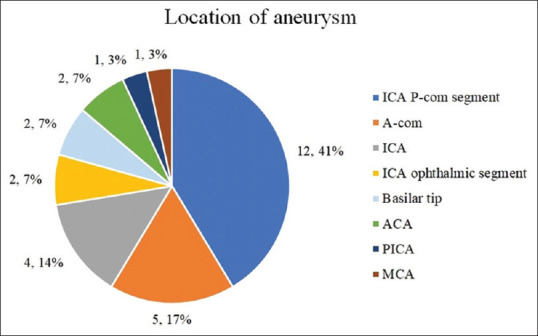
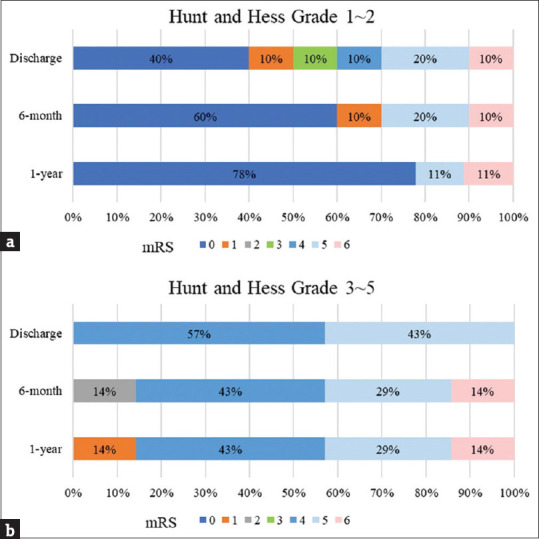
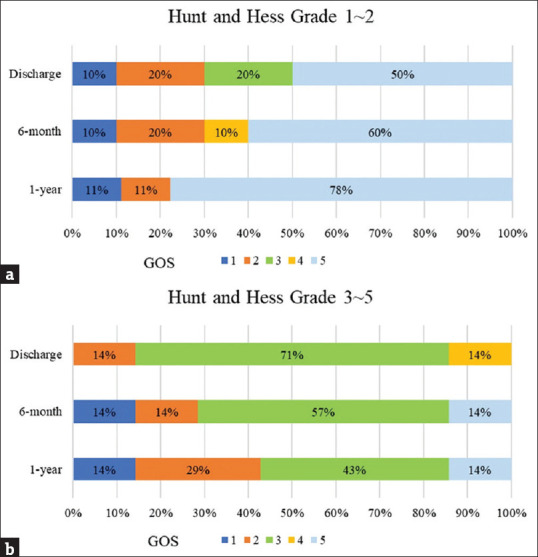
Results: Among the 17 patients included in this study, there were 14 (82.4%) women and 3 (17.6%) men, with a mean age of 58.59 years (standard deviation = 13.57; range: 40-82 years). There were no periprocedural hemorrhagic complications and no aneurysm rebleeding before discharge. However, two patients developed acute brain infarction because of symptomatic vasospasm. Linear regression revealed significant associations of posterior circulation involvement with the Glasgow Outcome Score and modified Rankin Scale (mRS) at discharge and 6 months after. Besides, Hunt and Hess grade ≥3 has a significant association with mRS at discharge, 6 months, and 1 year after.
Conclusion: SAC for ruptured aneurysm was technically feasible and did not carry an additional risk of postoperative aneurysm rebleeding secondary to antiplatelet treatment. Moreover, it had relatively low rates of aneurysm regrowth and coil compaction. Therefore, it can be a safe and effective endovascular treatment for acutely ruptured intracranial aneurysm.
期刊介绍:
The Tzu Chi Medical Journal is the peer-reviewed publication of the Buddhist Compassion Relief Tzu Chi Foundation, and includes original research papers on clinical medicine and basic science, case reports, clinical pathological pages, and review articles.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:



