Ryan Beerling Dolovac, James King, Christopher Ovenden, Jeremy Kam, Yi Yuen Wang, Tony Goldschlager, Mendel Castle-Kirszbaum
{"title":"鞍底重建对Rathke裂隙囊肿复发的影响:一项系统回顾和荟萃分析。","authors":"Ryan Beerling Dolovac, James King, Christopher Ovenden, Jeremy Kam, Yi Yuen Wang, Tony Goldschlager, Mendel Castle-Kirszbaum","doi":"10.1007/s11102-025-01521-4","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The optimal surgical technique for managing Rathke's Cleft Cyst (RCC) remains unclear. Leaving the sellar defect open (marsupialisation) after transsphenoidal surgery facilitates ongoing drainage of cyst contents, but cannot be performed in the setting of an intraoperative cerebrospinal fluid (CSF) leak. The effects of intraoperative CSF leaks and sellar floor reconstruction on RCC recurrence require further investigation.</p><p><strong>Methods: </strong>A systematic literature search was conducted for studies reporting RCC recurrence following transsphenoidal surgery, with data on intraoperative CSF leak rates and skull base reconstruction. Studies were classified based on surgical technique: cyst wall resection vs. fenestration, and open (no reconstruction) vs. closed (reconstructed) sellar floor.</p><p><strong>Results: </strong>Nineteen studies, comprising 1,076 patients, were included. The overall radiological RCC recurrence rate was 19.8% over a mean follow-up of 50.4 months. The recurrence rate in closed sella surgeries was significantly higher (32.1%) than in open sellar cases (14.0%) (OR 2.28, 95% CI: 1.41-3.67, p < 0.05). Intraoperative CSF leak occurred in 29.1% of cases. Patients with CSF leaks had a higher recurrence rate (23.4% vs. 12.9%), though meta-analysis demonstrated only a non-significant trend (OR 1.67, 95% CI: 0.95-2.96). Subgroup analysis revealed that intraoperative CSF leaks were significantly associated with increased recurrence after fenestration (38.5% vs. 18.4%, p = 0.03), and cyst wall resection (21.7% vs. 7.8%, p = 0.004). In the setting of an intraoperative CSF leak, there was a trend for lower recurrence when cyst wall resection was attempted (21.7% vs. 38.5%, p = 0.09).</p><p><strong>Conclusion: </strong>Patients undergoing transsphenoidal surgery for RCC experience high rates of postoperative radiological recurrence. Cyst fenestration while maintaining an open sellar floor (marsupialisation into the sphenoid sinus) is associated with a significantly lower risk of recurrence at over 4 years follow-up. Intraoperative CSF leaks were less strongly associated with cyst recurrence, suggesting that watertight reconstruction, rather than the leak itself, is the primary driver of reaccumulation. When a closed sella is necessitated by intraoperative CSF leak, the addition of cyst wall resection may be associated with a lower rate of recurrence than fenestration alone but must be weighed against a higher risk of AVP-deficiency.</p>","PeriodicalId":20202,"journal":{"name":"Pituitary","volume":"28 3","pages":"49"},"PeriodicalIF":3.4000,"publicationDate":"2025-04-14","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11996996/pdf/","citationCount":"0","resultStr":"{\"title\":\"Impact of sella floor reconstruction on Rathke Cleft Cyst recurrence: a systematic review and meta-analysis.\",\"authors\":\"Ryan Beerling Dolovac, James King, Christopher Ovenden, Jeremy Kam, Yi Yuen Wang, Tony Goldschlager, Mendel Castle-Kirszbaum\",\"doi\":\"10.1007/s11102-025-01521-4\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>The optimal surgical technique for managing Rathke's Cleft Cyst (RCC) remains unclear. Leaving the sellar defect open (marsupialisation) after transsphenoidal surgery facilitates ongoing drainage of cyst contents, but cannot be performed in the setting of an intraoperative cerebrospinal fluid (CSF) leak. The effects of intraoperative CSF leaks and sellar floor reconstruction on RCC recurrence require further investigation.</p><p><strong>Methods: </strong>A systematic literature search was conducted for studies reporting RCC recurrence following transsphenoidal surgery, with data on intraoperative CSF leak rates and skull base reconstruction. Studies were classified based on surgical technique: cyst wall resection vs. fenestration, and open (no reconstruction) vs. closed (reconstructed) sellar floor.</p><p><strong>Results: </strong>Nineteen studies, comprising 1,076 patients, were included. The overall radiological RCC recurrence rate was 19.8% over a mean follow-up of 50.4 months. The recurrence rate in closed sella surgeries was significantly higher (32.1%) than in open sellar cases (14.0%) (OR 2.28, 95% CI: 1.41-3.67, p < 0.05). Intraoperative CSF leak occurred in 29.1% of cases. Patients with CSF leaks had a higher recurrence rate (23.4% vs. 12.9%), though meta-analysis demonstrated only a non-significant trend (OR 1.67, 95% CI: 0.95-2.96). Subgroup analysis revealed that intraoperative CSF leaks were significantly associated with increased recurrence after fenestration (38.5% vs. 18.4%, p = 0.03), and cyst wall resection (21.7% vs. 7.8%, p = 0.004). In the setting of an intraoperative CSF leak, there was a trend for lower recurrence when cyst wall resection was attempted (21.7% vs. 38.5%, p = 0.09).</p><p><strong>Conclusion: </strong>Patients undergoing transsphenoidal surgery for RCC experience high rates of postoperative radiological recurrence. Cyst fenestration while maintaining an open sellar floor (marsupialisation into the sphenoid sinus) is associated with a significantly lower risk of recurrence at over 4 years follow-up. Intraoperative CSF leaks were less strongly associated with cyst recurrence, suggesting that watertight reconstruction, rather than the leak itself, is the primary driver of reaccumulation. When a closed sella is necessitated by intraoperative CSF leak, the addition of cyst wall resection may be associated with a lower rate of recurrence than fenestration alone but must be weighed against a higher risk of AVP-deficiency.</p>\",\"PeriodicalId\":20202,\"journal\":{\"name\":\"Pituitary\",\"volume\":\"28 3\",\"pages\":\"49\"},\"PeriodicalIF\":3.4000,\"publicationDate\":\"2025-04-14\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11996996/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Pituitary\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s11102-025-01521-4\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"ENDOCRINOLOGY & METABOLISM\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pituitary","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s11102-025-01521-4","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
Impact of sella floor reconstruction on Rathke Cleft Cyst recurrence: a systematic review and meta-analysis.
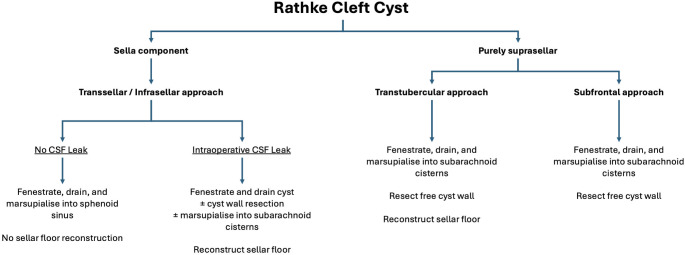
Background: The optimal surgical technique for managing Rathke's Cleft Cyst (RCC) remains unclear. Leaving the sellar defect open (marsupialisation) after transsphenoidal surgery facilitates ongoing drainage of cyst contents, but cannot be performed in the setting of an intraoperative cerebrospinal fluid (CSF) leak. The effects of intraoperative CSF leaks and sellar floor reconstruction on RCC recurrence require further investigation.
Methods: A systematic literature search was conducted for studies reporting RCC recurrence following transsphenoidal surgery, with data on intraoperative CSF leak rates and skull base reconstruction. Studies were classified based on surgical technique: cyst wall resection vs. fenestration, and open (no reconstruction) vs. closed (reconstructed) sellar floor.
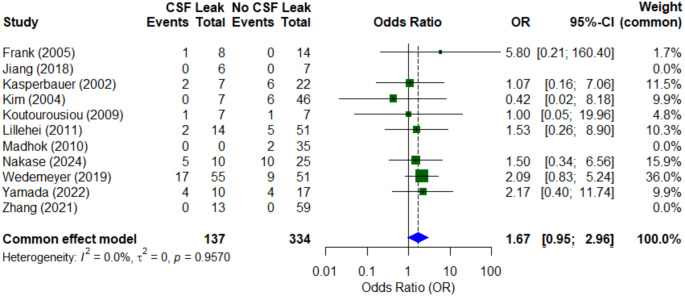
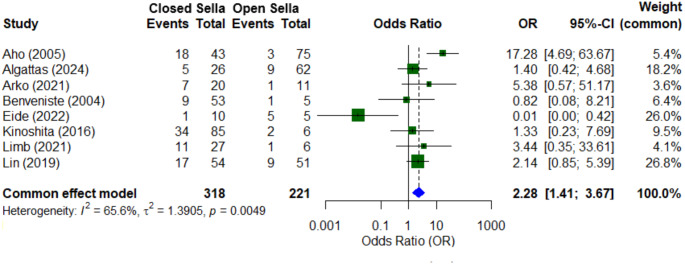
Results: Nineteen studies, comprising 1,076 patients, were included. The overall radiological RCC recurrence rate was 19.8% over a mean follow-up of 50.4 months. The recurrence rate in closed sella surgeries was significantly higher (32.1%) than in open sellar cases (14.0%) (OR 2.28, 95% CI: 1.41-3.67, p < 0.05). Intraoperative CSF leak occurred in 29.1% of cases. Patients with CSF leaks had a higher recurrence rate (23.4% vs. 12.9%), though meta-analysis demonstrated only a non-significant trend (OR 1.67, 95% CI: 0.95-2.96). Subgroup analysis revealed that intraoperative CSF leaks were significantly associated with increased recurrence after fenestration (38.5% vs. 18.4%, p = 0.03), and cyst wall resection (21.7% vs. 7.8%, p = 0.004). In the setting of an intraoperative CSF leak, there was a trend for lower recurrence when cyst wall resection was attempted (21.7% vs. 38.5%, p = 0.09).
Conclusion: Patients undergoing transsphenoidal surgery for RCC experience high rates of postoperative radiological recurrence. Cyst fenestration while maintaining an open sellar floor (marsupialisation into the sphenoid sinus) is associated with a significantly lower risk of recurrence at over 4 years follow-up. Intraoperative CSF leaks were less strongly associated with cyst recurrence, suggesting that watertight reconstruction, rather than the leak itself, is the primary driver of reaccumulation. When a closed sella is necessitated by intraoperative CSF leak, the addition of cyst wall resection may be associated with a lower rate of recurrence than fenestration alone but must be weighed against a higher risk of AVP-deficiency.
期刊介绍:
Pituitary is an international publication devoted to basic and clinical aspects of the pituitary gland. It is designed to publish original, high quality research in both basic and pituitary function as well as clinical pituitary disease.
The journal considers:
Biology of Pituitary Tumors
Mechanisms of Pituitary Hormone Secretion
Regulation of Pituitary Function
Prospective Clinical Studies of Pituitary Disease
Critical Basic and Clinical Reviews
Pituitary is directed at basic investigators, physiologists, clinical adult and pediatric endocrinologists, neurosurgeons and reproductive endocrinologists interested in the broad field of the pituitary and its disorders. The Editorial Board has been drawn from international experts in basic and clinical endocrinology. The journal offers a rapid turnaround time for review of manuscripts, and the high standard of the journal is maintained by a selective peer-review process which aims to publish only the highest quality manuscripts. Pituitary will foster the publication of creative scholarship as it pertains to the pituitary and will provide a forum for basic scientists and clinicians to publish their high quality pituitary-related work.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


