{"title":"应该给多少速尿来防止输血相关的循环负荷?一项剂量研究的结果。","authors":"Lianne Rotin, Liying Zhang, Chantal Armali, Amie Malkin, Sophia Massin, Harley Meirovich, Daniel Roque, Samia Saeed, Shangari Vijenthira, Yulia Lin, Jacob Pendergrast","doi":"10.1111/vox.70038","DOIUrl":null,"url":null,"abstract":"<p><strong>Background and objectives: </strong>Transfusion-associated circulatory overload (TACO) is a common and life-threatening transfusion complication. Because of uncertainty regarding dosing, pre-transfusion furosemide prophylaxis is not widely endorsed. The aim of this study was to generate a furosemide dose-response curve in TACO-susceptible patients using the multiple comparisons procedure and modelling (MCP-Mod) methodology.</p><p><strong>Materials and methods: </strong>Inpatients aged ≥50 years receiving intravenous (IV) furosemide were screened for eligibility at two academic hospitals. Exclusion criteria were active bleeding, haemodynamic instability, glomerular filtration rate (GFR) < 30 mL/min/1.73 m<sup>2</sup> and diuretic therapy administered within 24 h or albumin administered within 8 h. The primary outcome measure was 6-h urine output post furosemide administration. After incorporation of age, sex, chronic diuretic use, mean arterial pressure, GFR and serum albumin as covariates of diuretic response, MCP-Mod was applied after every 50th enrolment until a weight-adjusted dose-response curve was identified with 100 mL precision.</p><p><strong>Results: </strong>One-hundred forty-nine patients were enrolled. Urine output varied widely at each furosemide dose. Because of the presence of outliers and a paucity of patients receiving higher doses, only those receiving doses up to 0.6 mg/kg (n = 132) were included. After incorporating covariates, linear-log was identified as the best fitting model. Application of this formula revealed that, depending upon patient characteristics, 10-40 mg of furosemide IV would be required to achieve a diuresis volume of 400 mL, which is sufficient to offset 1 red blood cell unit.</p><p><strong>Conclusion: </strong>We report a novel furosemide dose-response model for TACO-susceptible patients. Once validated, this model will guide furosemide dosing for a planned controlled trial evaluating furosemide for TACO prevention.</p>","PeriodicalId":23631,"journal":{"name":"Vox Sanguinis","volume":" ","pages":"683-693"},"PeriodicalIF":1.6000,"publicationDate":"2025-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12286670/pdf/","citationCount":"0","resultStr":"{\"title\":\"How much furosemide should be administered to prevent transfusion-associated circulatory overload? Results of a dose-finding study.\",\"authors\":\"Lianne Rotin, Liying Zhang, Chantal Armali, Amie Malkin, Sophia Massin, Harley Meirovich, Daniel Roque, Samia Saeed, Shangari Vijenthira, Yulia Lin, Jacob Pendergrast\",\"doi\":\"10.1111/vox.70038\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background and objectives: </strong>Transfusion-associated circulatory overload (TACO) is a common and life-threatening transfusion complication. Because of uncertainty regarding dosing, pre-transfusion furosemide prophylaxis is not widely endorsed. The aim of this study was to generate a furosemide dose-response curve in TACO-susceptible patients using the multiple comparisons procedure and modelling (MCP-Mod) methodology.</p><p><strong>Materials and methods: </strong>Inpatients aged ≥50 years receiving intravenous (IV) furosemide were screened for eligibility at two academic hospitals. Exclusion criteria were active bleeding, haemodynamic instability, glomerular filtration rate (GFR) < 30 mL/min/1.73 m<sup>2</sup> and diuretic therapy administered within 24 h or albumin administered within 8 h. The primary outcome measure was 6-h urine output post furosemide administration. After incorporation of age, sex, chronic diuretic use, mean arterial pressure, GFR and serum albumin as covariates of diuretic response, MCP-Mod was applied after every 50th enrolment until a weight-adjusted dose-response curve was identified with 100 mL precision.</p><p><strong>Results: </strong>One-hundred forty-nine patients were enrolled. Urine output varied widely at each furosemide dose. Because of the presence of outliers and a paucity of patients receiving higher doses, only those receiving doses up to 0.6 mg/kg (n = 132) were included. After incorporating covariates, linear-log was identified as the best fitting model. Application of this formula revealed that, depending upon patient characteristics, 10-40 mg of furosemide IV would be required to achieve a diuresis volume of 400 mL, which is sufficient to offset 1 red blood cell unit.</p><p><strong>Conclusion: </strong>We report a novel furosemide dose-response model for TACO-susceptible patients. Once validated, this model will guide furosemide dosing for a planned controlled trial evaluating furosemide for TACO prevention.</p>\",\"PeriodicalId\":23631,\"journal\":{\"name\":\"Vox Sanguinis\",\"volume\":\" \",\"pages\":\"683-693\"},\"PeriodicalIF\":1.6000,\"publicationDate\":\"2025-07-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12286670/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Vox Sanguinis\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1111/vox.70038\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/4/29 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"HEMATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Vox Sanguinis","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1111/vox.70038","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/4/29 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"HEMATOLOGY","Score":null,"Total":0}
How much furosemide should be administered to prevent transfusion-associated circulatory overload? Results of a dose-finding study.
Background and objectives: Transfusion-associated circulatory overload (TACO) is a common and life-threatening transfusion complication. Because of uncertainty regarding dosing, pre-transfusion furosemide prophylaxis is not widely endorsed. The aim of this study was to generate a furosemide dose-response curve in TACO-susceptible patients using the multiple comparisons procedure and modelling (MCP-Mod) methodology.
Materials and methods: Inpatients aged ≥50 years receiving intravenous (IV) furosemide were screened for eligibility at two academic hospitals. Exclusion criteria were active bleeding, haemodynamic instability, glomerular filtration rate (GFR) < 30 mL/min/1.73 m2 and diuretic therapy administered within 24 h or albumin administered within 8 h. The primary outcome measure was 6-h urine output post furosemide administration. After incorporation of age, sex, chronic diuretic use, mean arterial pressure, GFR and serum albumin as covariates of diuretic response, MCP-Mod was applied after every 50th enrolment until a weight-adjusted dose-response curve was identified with 100 mL precision.
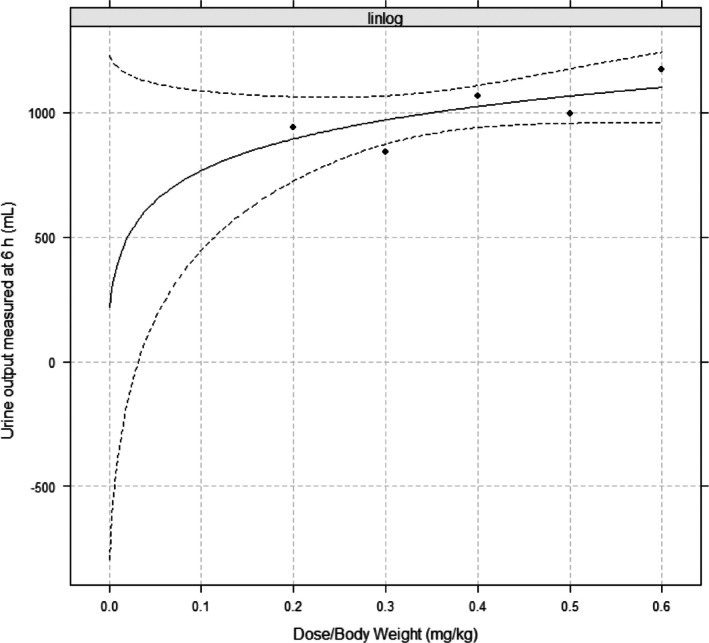
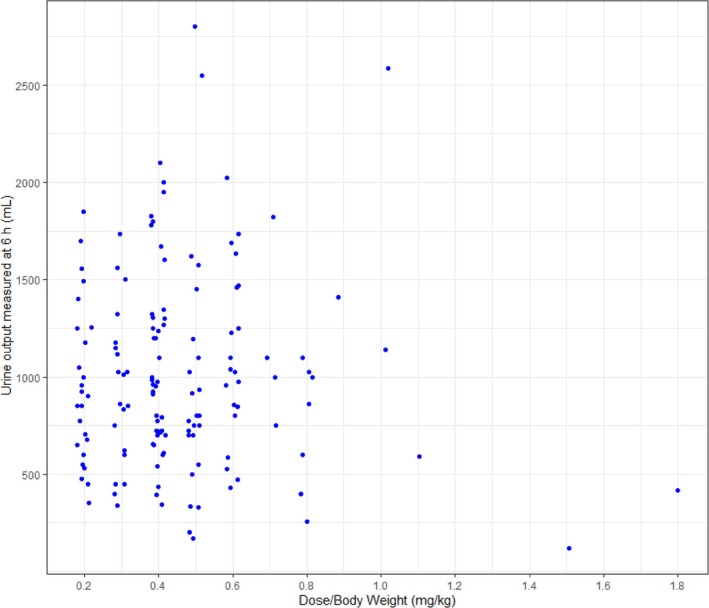
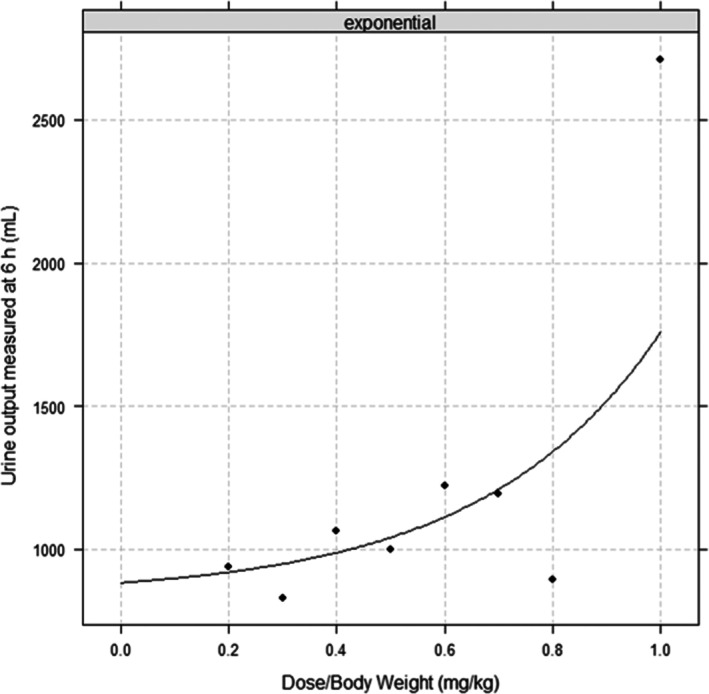
Results: One-hundred forty-nine patients were enrolled. Urine output varied widely at each furosemide dose. Because of the presence of outliers and a paucity of patients receiving higher doses, only those receiving doses up to 0.6 mg/kg (n = 132) were included. After incorporating covariates, linear-log was identified as the best fitting model. Application of this formula revealed that, depending upon patient characteristics, 10-40 mg of furosemide IV would be required to achieve a diuresis volume of 400 mL, which is sufficient to offset 1 red blood cell unit.
Conclusion: We report a novel furosemide dose-response model for TACO-susceptible patients. Once validated, this model will guide furosemide dosing for a planned controlled trial evaluating furosemide for TACO prevention.
期刊介绍:
Vox Sanguinis reports on important, novel developments in transfusion medicine. Original papers, reviews and international fora are published on all aspects of blood transfusion and tissue transplantation, comprising five main sections:
1) Transfusion - Transmitted Disease and its Prevention:
Identification and epidemiology of infectious agents transmissible by blood;
Bacterial contamination of blood components;
Donor recruitment and selection methods;
Pathogen inactivation.
2) Blood Component Collection and Production:
Blood collection methods and devices (including apheresis);
Plasma fractionation techniques and plasma derivatives;
Preparation of labile blood components;
Inventory management;
Hematopoietic progenitor cell collection and storage;
Collection and storage of tissues;
Quality management and good manufacturing practice;
Automation and information technology.
3) Transfusion Medicine and New Therapies:
Transfusion thresholds and audits;
Haemovigilance;
Clinical trials regarding appropriate haemotherapy;
Non-infectious adverse affects of transfusion;
Therapeutic apheresis;
Support of transplant patients;
Gene therapy and immunotherapy.
4) Immunohaematology and Immunogenetics:
Autoimmunity in haematology;
Alloimmunity of blood;
Pre-transfusion testing;
Immunodiagnostics;
Immunobiology;
Complement in immunohaematology;
Blood typing reagents;
Genetic markers of blood cells and serum proteins: polymorphisms and function;
Genetic markers and disease;
Parentage testing and forensic immunohaematology.
5) Cellular Therapy:
Cell-based therapies;
Stem cell sources;
Stem cell processing and storage;
Stem cell products;
Stem cell plasticity;
Regenerative medicine with cells;
Cellular immunotherapy;
Molecular therapy;
Gene therapy.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


