Giuliana Vespere, Silvia Sedda, Pasquale Madonna, Roberta Abete, Alfredo D'Avino, Manuela Maione, Marina Lugarà, Antonietta Tazza, Franco Scaldaferri, Giuseppe Vitiello, Leonardo De Luca
{"title":"非戈替尼治疗急性严重难治性溃疡性结肠炎1例报告及文献复习。","authors":"Giuliana Vespere, Silvia Sedda, Pasquale Madonna, Roberta Abete, Alfredo D'Avino, Manuela Maione, Marina Lugarà, Antonietta Tazza, Franco Scaldaferri, Giuseppe Vitiello, Leonardo De Luca","doi":"10.1159/000545263","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Acute severe ulcerative colitis (ASUC) is a serious complication affecting 9%-15% of patients with UC within 3 months of diagnosis and up to 28% of patients during the course of the disease. Despite the use of infliximab and calcineurin inhibitors, the rate of colectomy remains high both during the hospitalization and in the 5 years after an acute episode. We present a case of ASUC that was unresponsive to conventional therapies but was successfully treated with filgotinib.</p><p><strong>Case presentation: </strong>A 21-year-old male with a recent diagnosis of UC presented to our hospital with a severe flare. He received rescue therapy of high-dose intravenous steroids and 10 mg/kg infliximab. We observed little clinical and biochemical benefits. The patient declined the surgical option. Therefore, we decided to start a second rescue therapy with a new and rapid-acting Janus kinase inhibitor, filgotinib, due to its characteristics and pharmacokinetic profile of rapid absorption and metabolism. The patient showed an immediate clinical and biochemical response at 48 h, an endoscopic response at week 3, and an endoscopic remission at week 10. No recurrence was observed after 12 months of follow-up. The patient is in clinical remission with a good quality of life.</p><p><strong>Conclusion: </strong>Filgotinib may be an effective second-line therapy in an emergency setting such as ASUC in patients unresponsive to conventional therapy.</p>","PeriodicalId":9614,"journal":{"name":"Case Reports in Gastroenterology","volume":"19 1","pages":"289-297"},"PeriodicalIF":0.6000,"publicationDate":"2025-04-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12028979/pdf/","citationCount":"0","resultStr":"{\"title\":\"Filgotinib to Treat Acute Severe Refractory Ulcerative Colitis: A Case Report and Review of the Literature.\",\"authors\":\"Giuliana Vespere, Silvia Sedda, Pasquale Madonna, Roberta Abete, Alfredo D'Avino, Manuela Maione, Marina Lugarà, Antonietta Tazza, Franco Scaldaferri, Giuseppe Vitiello, Leonardo De Luca\",\"doi\":\"10.1159/000545263\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Acute severe ulcerative colitis (ASUC) is a serious complication affecting 9%-15% of patients with UC within 3 months of diagnosis and up to 28% of patients during the course of the disease. Despite the use of infliximab and calcineurin inhibitors, the rate of colectomy remains high both during the hospitalization and in the 5 years after an acute episode. We present a case of ASUC that was unresponsive to conventional therapies but was successfully treated with filgotinib.</p><p><strong>Case presentation: </strong>A 21-year-old male with a recent diagnosis of UC presented to our hospital with a severe flare. He received rescue therapy of high-dose intravenous steroids and 10 mg/kg infliximab. We observed little clinical and biochemical benefits. The patient declined the surgical option. Therefore, we decided to start a second rescue therapy with a new and rapid-acting Janus kinase inhibitor, filgotinib, due to its characteristics and pharmacokinetic profile of rapid absorption and metabolism. The patient showed an immediate clinical and biochemical response at 48 h, an endoscopic response at week 3, and an endoscopic remission at week 10. No recurrence was observed after 12 months of follow-up. The patient is in clinical remission with a good quality of life.</p><p><strong>Conclusion: </strong>Filgotinib may be an effective second-line therapy in an emergency setting such as ASUC in patients unresponsive to conventional therapy.</p>\",\"PeriodicalId\":9614,\"journal\":{\"name\":\"Case Reports in Gastroenterology\",\"volume\":\"19 1\",\"pages\":\"289-297\"},\"PeriodicalIF\":0.6000,\"publicationDate\":\"2025-04-25\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12028979/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Case Reports in Gastroenterology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1159/000545263\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q4\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Gastroenterology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1159/000545263","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
Filgotinib to Treat Acute Severe Refractory Ulcerative Colitis: A Case Report and Review of the Literature.
Introduction: Acute severe ulcerative colitis (ASUC) is a serious complication affecting 9%-15% of patients with UC within 3 months of diagnosis and up to 28% of patients during the course of the disease. Despite the use of infliximab and calcineurin inhibitors, the rate of colectomy remains high both during the hospitalization and in the 5 years after an acute episode. We present a case of ASUC that was unresponsive to conventional therapies but was successfully treated with filgotinib.
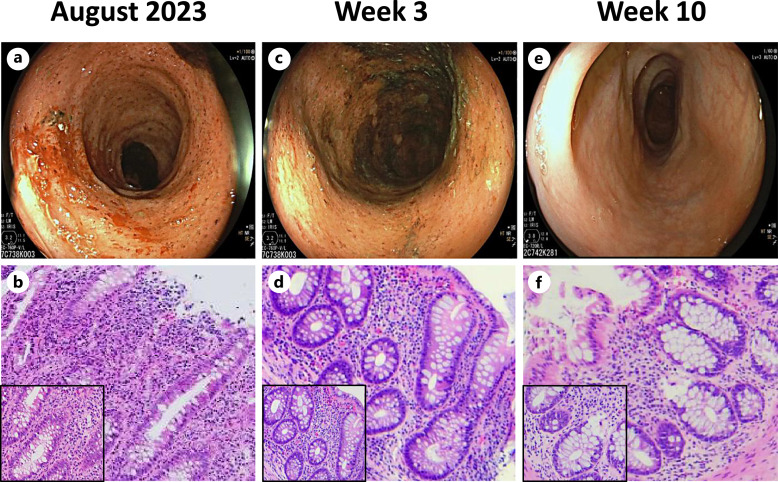
Case presentation: A 21-year-old male with a recent diagnosis of UC presented to our hospital with a severe flare. He received rescue therapy of high-dose intravenous steroids and 10 mg/kg infliximab. We observed little clinical and biochemical benefits. The patient declined the surgical option. Therefore, we decided to start a second rescue therapy with a new and rapid-acting Janus kinase inhibitor, filgotinib, due to its characteristics and pharmacokinetic profile of rapid absorption and metabolism. The patient showed an immediate clinical and biochemical response at 48 h, an endoscopic response at week 3, and an endoscopic remission at week 10. No recurrence was observed after 12 months of follow-up. The patient is in clinical remission with a good quality of life.
Conclusion: Filgotinib may be an effective second-line therapy in an emergency setting such as ASUC in patients unresponsive to conventional therapy.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


